![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
|
What is Subungual hematoma? |

Subungual hematoma: - bleeding underneath toe nails - common in distance running - secondary to deceleration - toe hits end of toe box and causes disruption in nail/toe bed - can be acute (drop a weight, step on) |
|
|
Subungual hematoma treatment. |
Subungual hematoma treatment - evacuate blood to v pressure - sterile heated paper clip --> user pliers to hold clip --> press into nail --> blood will release - manual pressure on nail to evacuate blood and then Band-Aid - old nail falls off, new nail will grow |
|
|
Subungual hematoma prevention. |
Subungual hematoma prevention. a) pad end of shoes b) get bigger shoes c) cut toe nails shorter d) pad forefoot (holds your foot back so your toe doesn't bang on the end of the toe)
|
|
|
Describe an ingrown toenail. |
Ingrown toenail - usually big toe - nail grows into lateral nail fold - usually from lateral pressure of poorly fitting shoes, improper trimming or repeated trauma - tissue being pushed over the nail (nail to wide) - if bacteria gets under sterile max = infection (anaerobic bacteria causes yellow puss & smell)
|
|
|
Ingrown toenail treatment. |
Ingrown toenail treatment - soak in warm water (to make tissues soft & pliable) - tease tissue back from nail - tuck cotton along border of nail, blot out excessive moisture & trim - twice a day until inflammation settles - allow nail to grow just beyond toe & cut small v shape in nail (stress relief point in nail) |
|
|
Ingrown toenail prevention. |
Ingrown toenail prevention proper trimming - trim weekly by cutting straight across - avoid rounding so margins do not penetrate the tissues on the side - long enough to clear underlying skin (usually people cut too short) |
|
|
Where does the stability come from to support the ankle joint? |
Stability comes from: 1. shape of bones 2. capsule & ligaments 3. strength of muscles |
|
|
How does the shape of the bones create stability for the ankle joint? |
Bony ankle joint Talocrural joint/mortise - latteral malleous longer & more posterior than medial: GIVES A LOT OF STABILITY |
|
|
Is the ankle more stable in plantar flexion or in dorsi flexion? Why? |
- plantar flex: space in joint (less stable) - dorsi flex: joint space is full (more stable)
This is because the trochlear surface is wider anteriorly than posteriorly
|
|
|
How does the joint capsule increase ankle stability? |
Joint capsule - ankle surrounded by fibrous capsule - thin and weak anteriorly & posteriorly to allow movement - strengthened medial & laterally by ligaments |
|
|
Describe the roles of the ATFL, CFL and PTFL in increasing ankle stability. |
Ligaments ATFL (anterior talo-fibular ligament) - weakest of 3 lateral ligaments - strain ^ with plantar flexion/inversion - part of capsule
CFL (calcaneo-fibular ligament) - stabilizes sub talar joint and limits adduction /medial tit - tight in neutral dorsiflexion - not part of capsule
PTFL (posterior talo-fibular ligament) - strongest of all lateral ligaments
- capsular ligament: swell - non capsular ligament: no swelling
|
|
|
When do ankle sprains occur? (Loading or unloading) |
Ankle sprain occur when unloading because less stable - mortise is a loose fit |
|

What ligament is the first line of defense for each image? |
The most vertical ligament will be the first line of defence, it gets the most stretched
a) plantar flexion - talo-fibular ligament
b) neutral - calcaneo-fibular ligament
c) dorsiflexion - calcaneo-fibular ligament |
|
|
What is the anterior drawer test? (Ankle stability test) |
Anterior drawer test - determine damage to anterior talo-fibular ligament - positive test: foot slides forward and/or makes a clunking sound as it reaches end point |
|
|
What are you looking for during a ligament test? |
Ligament tests, looking for: - end pt - laxity - pain |
|
|
What is the talar tilt test? (Ankle stability test) |
Talar tilt test: - determine damage to the calcaneo-fibular ligament (inversion) or deltoid ligament (eversion) - positive test: if there is excess motion/pain when the foot is inverted/everted at 90 degrees |
|
|
Describe the deltoid ligament. |
Deltoid ligament - medial - superficial - limits talar abduction/lateral tilt
- anterior part: tight in plantar flexion & eversion - middle part: neutral - posterior part: tight in dorsiflexion |
|
|
Describe an eversion ankle sprain. |
Eversion sprain - least common sprain - most fractures happen - stability of medial ankle depends on deltoid ligament & lateral malleolus
- medial tenderness - ^ pronation (ligament holding up the search is torn, so foot drops into an ^ pronation)
|
|
|
What are the 3 phases of the ligament load-deformation curve? |
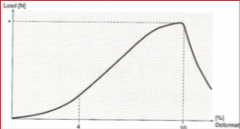
3 phases of load-deformation curve: - toe region - linear region - rupture region |
|
|
What is the Ottawa Ankle Rule? |
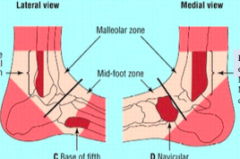
Ottawa Ankle Rules - decide if you need to send someone for an x ray - want to spend less money on x rays
pain at any of these 4 spots or can't walk (testing for fractures) a) posterior edge or tip of lateral malleolus b)posterior edge or tip of medial malleolus c) base of fifth metatarsal d) navicular
|
|
|
What is generally injured during over eversion & external rotation? |
Over eversion & external rotation 1. deltoid ligaments 2. anterior inferior tibio-fibular ligament 3. fracture in the lateral side of fibula |
|
|
What is the external rotation test? |
External rotation test - externally rotate foot, pain high up on leg |
|
|
What is the order of assessment flow? |
Assessment flow 1. subjective 2. objective 3. AROM 4. PROM 5. resisted movements |
|
|
What happens during the subjective assessment? |
Subjective - what was the mechanism of injury?(inversion/eversion, dorsiflexed/plantar-flexed) - where you able to continue? (can't bear weight: sig injury, able to walk: gr 2, able to run: gr 1) - did you hear/feel a pop or crack - did it swell? how quickly? (capsular vs non capsular) - how bad is pain? - what positions make it worse? |
|
|
What happens during the objective assessment? |
Objective - swelling - obvious deformity - weight bearing (static: equal pressure, dynamic: guarded movement)
|
|
|
What tests can be done to rule out a fracture? |
How to rule out a fracture: 1. Ottawa test 2. Squeeze test 3. External rotation test |
|
|
What are the special tests? |
Special tests: - manual muscle testing - talar tilt - anterior draw |