Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
27 Cards in this Set
- Front
- Back
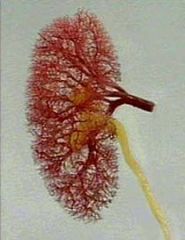
Normal Kidney
- EM |
|
|
|
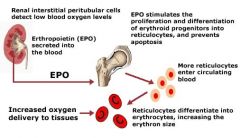
EPO
|
|
|
|
Vit D
|

|
|
|
Failing Kidneys
|
1. Toxins build up:
–Urea (nausea) –Potassium (weakness and heart rhythm) –Phosphate (itch, PTH and bone disease) –Acid (breathlessness and bone disease) 2. Water retention: –Fluid in the lungs (breathlessness) –Fluid in the legs (oedema) –High blood pressure +/- hormone effect 3. Erythropoietin deficiency: – Anaemia (tiredness, lack of energy, breathless) 4. Vitamin D deficiency: –Low calcium (pins and needles, cramps) –Bone disease (PTH, bone pain, factures) |
|
|
Simple assessment of kidney function
|
•Abnormal kidney function: Blood tests
–Increased urea –Increased creatinine –Increased potassium –Increased phosphate –Increased acid (low bicarbonate level, low pH) –Increased parathyroid hormone –Increased renin –Decreased haemoglobin (decreased erythropoietin) –Decreased calcium –Decreased vitamin D •Abnormal kidney function: Examination –Appearance: Pale (anaemic), sallow (uraemic) –Smell: uraemic fetor –Kussmaul’s respiration (metabolic acidosis) –Abnormal movement: asterixis –Hypertension –Fluid retention (peripheral/pulmonary oedema) |
|
|
Reviewing patients with specific abnormalities:
FORMAL KIDNEY PROBLEMS |
–Reduced GFR (abnormal creatinine)
–Proteinuria –Haematuria/pyuria/cast excretion –Hyperkalaemia/acid-base disturbance –Nocturia/frequency |
|
|
Purpose of renal function testing
|
1. review patients with specific kidney abnormalities
2. Monitor patients on nephrotoxic Tx –Lithium –Cyclosporin –Chemotherapy 3. Determine normal renal fn - kidney donor work up –Post partum following pre-eclampsia –Post nephrectomy |
|
|
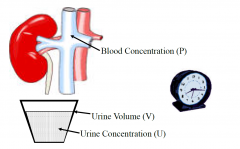
Renal clearance
|
•Is the measure of the ability of a kidney to clear a given substance
•Renal clearance is effected by: –Glomerular filtration –Tubular secretion –Tubular reabsorption –Metabolism •Main use is to determine glomerular filtration rate: our best estimate of “renal function” |
|
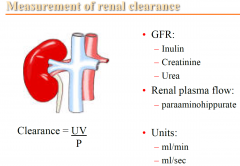
Measurement of renal clearance
|
|
|
|
Inulin
|
–Freely filtered by the glomerulus
–No tubular secretion or reabsorption –Best measure of GFR: impractical |
|
|
Creatinine
|
–Freely filtered by the glomerulus
–Some tubular secretion –Can overestimate the inulin GFR (10-20%) –Can be improved by using cimetidine |
|
|
Urea
|
–Freely filtered by the glomerulus
–Some tubular reabsorption –Underestimates the inulin GFR •Average of urea and creatinine clearance: –Can help adjust for the tubular effects |
|
|
•Paraaminohippurate (PAH):
|
–Freely filtered
–Active tubular secretion –Complete removal of the PAH from the plasma in a single pass of the kidney –Therefore is used as a measure of Renal Plasma Flow –Little clinical utility |
|
|
BSA
|
•Using Body Surface Area (BSA)
–e.g. DuBois and DuBois equation •Clearance = ml/min/1.73m2 •BSA of 1.73m2 considered to be average |
|
|
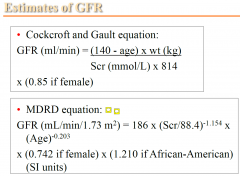
Estimates of GFR
|
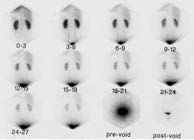
•Nuclear GFR
|
|
|
MDRD limitations
- eGFR |
only accurate in impaired renal function patients (because thats where oit was extrapolated from)
- so if normal its given in >60ml?min |
|
|
Nuclear GFR
|
|
|
|
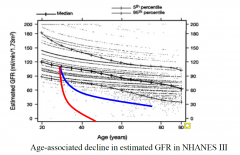
Relationship between GFR and Cr
|
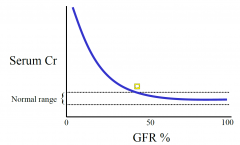
so not till below 50% is it not normal any more
NON-LINEAR |
|
|
Ageing and the Kidney
|
|
|

Urinary concentrating ability
tests |

•Tested using:
–Overnight water deprivation (from 10pm) –Maximised using synthetic ADH (intra-nasal) measure morning urine volume - give the ADH and test urine osmolality THIS PATIENT: impaired ability to concentrate (thus its not ADH dependednt but kidney problem) |
|

What is this called?
|
Nephrogenic diabetes Insipidus
|
|
|
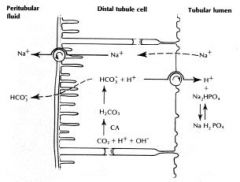
Acidification ability
Bicarbonate |
•Bicarbonate:
–Is freely filtered by the glomerulus –The MAJORITY is reabsorbed by the proximal convoluted tubules –Some is also reabsorbed by the distal tubules |
|
|
–Tubular disease can lead to excessive losses of bicarbonate and result in a systemic acidosis
Q: What name is given to this abnormality? |
A: Proximal renal tubular acidosis
|
|
|
Acid Excretion
|
•Acid:
–Is actively excreted into the urine in the distal tubule |
|
|
–Tubular disease can lead to excessive accumulation and result in a systemic acidosis
Q: What name is given to this abnormality? |
A: Distal renal tubular acidosis
|
|
|
•How to test for an acidification defect?
|
•Blood test:
– Acidosis (pH < 7.35) – Anion gap = Na - Cl - HCO3, (Normal 8-16) – Renal tubular disease: normal anion gap acidosis • Urine test: – Urinary pH – Urinary bicarbonate – Formal acidification study |
|
|
• Acidification test using oral ammonium chloride
|
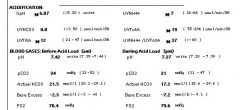
- ammonium chloride a weak acid
shouldve been 5.2 (thus the defect in acid excretion in the distal - i.e incomplete distal renla tubular acidosis) |