Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
61 Cards in this Set
- Front
- Back
|
cardiac causes of arrhythmias
|
MI
CAD LV aneurysm mitral valve disease cardiomyopathies pericarditis/ myocarditis aberrant conduction pathways |
|
|
non-cardiac causes of arrhythmias
|
smoking
alcohol pneumonia drugs (B-agonists, digoxin) metabolic imbalance (e.g. ↑/↓K+) |
|
|
2 drugs which can cause arrhythmias
|
digoxin
B-agonists |
|
|
presentation of arrhythmias
|
asymp/ incidental
palpilataions chest pain presyncope/ syncope hypotension po oedema dyspnoea |
|
|
Q's to ask in hx about arrhythmia
|
precipitating factors: emotional, weather, exercise
onset nature: fast/slow, reg/irreg duration & freq associated symptoms PMH DH FH (SH) |
|
|
2 origins of an arrhythmia
|
1) SVT (SA, atria, AV, His)
2) VENTRICULAR (muscle, fasciles of conducting system) |
|
|
3 types of SVT tachycardia
|
AF
atrial flutter ectopic atrial tachy |
|
|
2 types of SVT bradycardia
|
sinus bradycardia
sinus PAUSES |
|
|
4 types of ventricular arrhythmias (which 2 are deadly)
|
ventricular ectopics/ prem vent complexes (PVCs)
VT deadly!!: - VF - asystole |
|
|
3 arrythymais affecting the AV node
|
AVN re-entrant tachy (AVNRT)- left
AV reciprocating tachycardia (AVRT) - accessory pathyway- right AVN block (1st-3rd degree) |
|
|
the most common cardiac arrhythmia
|
AF
|
|
|
6 general types of causes of arrhythmias
|
structural abnormality (anatomy)
ANS metabolic inflammation (peri/myo-carditis) drugs (digoxin, B-agonists) genetic |
|
|
what's an ectopic beat:
what 2 reasons can it be due to? |
originate in place other than SA node
can be single or sustained - altered automaticity (ischaemia, metabolic) - triggered activity (drugs, ANS) |
|
|
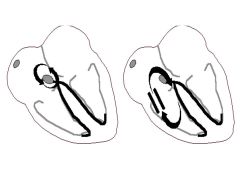
what's AVRT (AV reciprocating tachycardia);
- 3 causes |
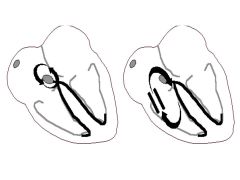
2+ conduction pathways (outwith normal purkinjie system)- pic on right
different speeds and refractioness self-perpetuating circuit - accessory pathways (WPW) - prev mi (ischaemia) - congenital |
|
|
in the ventricular myocyte AP, when can afterdepolarisations occur? (from an ectopic)
what term if given to sustained train of depolarisations |
in phase 3 repolarisation (↑K efflux)
...TRIGGERED activity |
|
|
what mechanism of electrical abnormality underlies DIGOXIN toxicity, torsades de pointes (long QT syndrome) & hypokalaemia?
(from an ectopic) |
TRIGGERED activity
sustained train of depolarisations in phase 3 mytocyte AP ↑QRS/ polymorphic VT on ECG |
|
|
5 Ix's for arrhythmias
|
FBC, U&Es, glucose, Ca, Mg
ECG: ?exercise test, ?24hr, event recoder Echo: structure ELECTROPHYSIOLOGICAL study: interventional (RFCA) CXR |
|
|
what does a delta wave on an ECG suggest- explain the syndrome
|
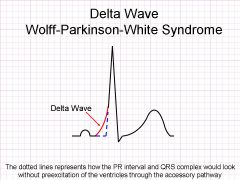
congenital accessory pathway between atria:ventricles
|
|
|
normal HR
|
70-100bmp
|
|
|
what sinus bradycardia
causes treatment |
<60bmp reg
physiological, drugs, ischaemia - ATROPINE (non-selective M antagonist of ACh)...widespread - PACING if haemodynamically unstable |
|
|
side effects of atropine
|
blocks parasym activation...widespread
✕ VF ✕ SVT ✕ dizzy, N&V, burred vision ✕ contraindicated in ischaemia |
|
|
what's sinus tachycardia
causes treatment |
>100bmp reg
physiological (pain, fever, ↑O2 demand) SE of drugs - underlying cause - BBs if inappropriate |
|
|
treatment/ management of atrial ectopic beats
|
NONE!
- BBs may help - avoid stimulants (caffeine, smoking) |
|
|
what's sinus arrhythmia
who treatment/ management |
phasic variation in HR with RESPIRATION
children & young adults aware of...NOT TREATED |
|
|
most common paroxysmal arrhythmia in children/ young adults:
pounding heart beat, breathless ECG- narrow complex tachycardia rate >100bpm |
SVTs
|
|
|
types of atrial and AVN mechanisms of SVTs
|
Atrial:
- AF/ atrial flutter/ ectopics AVN: - AVRT/ AVNRT/ ectopic |
|
|
morphology on ECG of SVT
|
>100bpm, reg, narrow QRS
|
|
|
treatment of acute SVT (i.e. paroxysmal)
|
vagogenic manoeuvres: valsalva
IV adenosine/ verapamil- slow AV conduction |
|
|
treatment of chronic SVTs
|
avoid stimulants
RFCA (during electrophysiological study) BBs |
|
|
causes of Av conduction diseases
|
infection/ rheumatic heart disease
age, alcohol, HTN AMI/ IHD druge: BBs, CCBs, digoxin valve disease/ surgery congenital |
|
|
identify 1st degree AV node block
management |
PR interval longer than normal >0.2s
no treatment |
|
|
identify 2nd degree heart block: mobitz type 1
treatment |

prolonged QRS, then drop a QRS & T
cyclic reg irreg NO TREATMENT |
|
|
identify 2nd degree heart block: mobitz type 2
treatment |

2 P : 1 QRS wave - fixed
reg irreg PACING |
|
|
identify 3rd degree heart block (complete)
treatment |
atria and ventricles beating indepentently
irreg PACING |
|
|
2 types of pacing
when are they used |
transcutaneous - emergency temp
transvenous- long-term |
|
|
indications for pacemaker (transcutaneous or transvenous)
|
heart block:
- 2nd deg mobitz 2 - 3rd deg (complete) |
|
|
what are PVC / ventricular ectopics
identify on ECG |
early ventricular contraction
followed by pause...then a forceful contraction ("palpitation") |
|
|
treatment of PVCs/ ventricular ectopics
|
BBs
RFCA (of focus/ foci) |
|
|
common cause(s) of VT
rarer causes |
significant heart disease (scar tissue): IHD, CAD, prev-MO
rare: cardiomyopathies, genetic, metabolic |
|
|
identify VT on a ECG
|
rate variable (fast 200+), Reg
distorted, wide QRS >0.1s, large inverted T waves, P not visible |
|
|
acute immediate treatment for VT (consider if unstable. stable or unsure of dx)
|
stable = pharmacological cardioversion (prep for DCCV)
unstable= DCCV unsure= adenosine |
|
|
long-term management/treatment of VT
|
correct ischaemia/ optimise CHF drugs
RFCA ICD (implantable cardiovertor defibs) - if life-threatening |
|
|
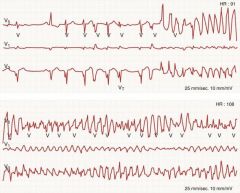
Identify VF on ECG and Pt!
|

incompatible with life- no CO!!!
v.fast 300-600bmp, irreg, CHAOTIC, absent P |
|
|
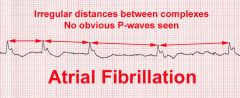
identify atrial fibrillation (AF) on a ECG
|
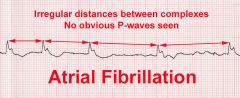
paroxysma;/ persistent/ permanent chaotic atrial activity.
Irreg irreg rhythm |
|
|
3 types and brief definition of AF
|
1) paroxysmal- <48hrs, recurrent
2) persistent- >48hrs, can be cardioverted 3) permanent- herat disease, NSR can't be restored! |
|
|
mechanism of AF
|
multiple ectopic foci/ reentry- usually located around po veins (LA)
|
|
|
3 ways of converting AF to NSR
|
pharmacological
electrical spontaneous |
|
|
what's lone AF
|
no cause- Dx of EXCLUSION
absence of any heart disease no ventricular dysfunction asymp ?genetic stroke risk |
|
|
complications of AF
|
THROMBOEBOLISM
Torsades De Pointes |
|
|
When are anti-coagulants indicated for AF
|
mitral valve disease
>75 HTN HF prev stroke/ thrmboembolism CAD/ DM |
|
|
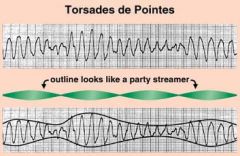
what's Torsades De Pointes
identify on ECG |
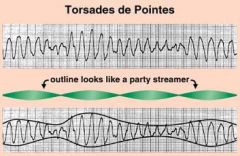
Deadly form of VT, HR 200-250, irreg
long QT & QRS, changing morphology |
|
|
what % treated AF pt's relapse within 1 year
|
70%
|
|
|
2 main pharmacological management aims in AF
one other important area of pharmacological treatment (secondary prevention) |
rate control
rhythm control antithrombotic therapy! (aspirin/ warfarin) |
|
|
antithrombotic therapy is given to pts with AF and atrial flutter. which drugs are used
|
aspirin (antiplatelet)
warfarin (anticoagulant) |
|
|
rhythm-control drug/ other methods used to cardiovert AF
|
AMIODARONE IV (anti-arrhythmic drug)
DCCV |
|
|
which pharmacological / and other, RATE-control methods used in treating AF
|
BBs
rate-limiting CCBs (verapamil, diltiazem) Digoxin RFCA |
|
|
4 classes of anti-arrhythmic drugs that target each phase of the myocyte AP (Now Can Kill Beats)
eg's |
0- Na blockers
2- CCBs (verapamil) 3- K blockers (AMIODARONE, sotalol) 4- BBs (bisiprolol, atenolol) |
|
|
identify atrial flutter on a ECG
|
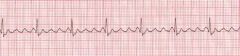
SAW TOOTH appearance
rapid, reg atrial tachy usually paroxysmal, macro-reentrant CLOCKWISE circuit in RA. chronic....AF |
|
|
mechanism of Atrial flutter
|
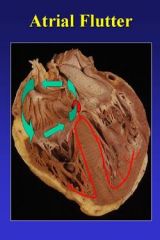
macro-reentrant circuit in RA
clockwise |
|
|
treatment/ management of atrial flutter
|
RFCA
pharmacological cardioversion electrical cardioversion (DCCV) WARFARIN - anticoagulant |
|
|
what's asystole
is it shockable treatment |
absent QRS
(atrial P waves may persist) NON-SHOCKABLE ADRENALINE |