Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
72 Cards in this Set
- Front
- Back
|
LV mass (weight) remains normal in?
a) ar b) as c) mr d) ms |
ms
|
|
|
What false positive can high angulation of mmode transducer beam result in?
|
pseudo bicuspid aortic valve
|
|
|
What is the primary effect of long-standing ar?
|
decreased ef
|
|
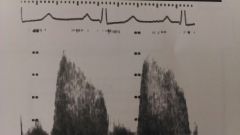
Is this spectral trace MS or AI?
|
AI because it's high velocity (4 m/sec)
|
|
|
What does RVSP equal?
|
PAP
|
|
|
Describe Lambl's Excrescences
|
thin filiform strands on edges of valve leaflets
|
|
|
What causes a pericardial knock?
|
abrupt cessation of early diastolic inflow
|
|
|
When do you hear pericardial knock?
|
in constrictive pericarditis
|
|
|
What often accompanies bicuspid av and how often?
|
coarc
50% |
|
|
When is MV pressure half time not accurate?
|
after balloon valvuloplasty
|
|
|
Given TR and RA pressures, what can you calculate?
|
RVSP
|
|
|
If patient has diliated LV and thin septum, what is going on?
|
severe MR
|
|
|
What is best way to determine severity of MR?
|
pulmonary venous flow
|
|
|
Name two layers of pericardium
|
visceral and parietal
|
|
|
Which cardiac pathology affects the valves?
|
carcinoid
|
|
|
Which pericardial layer is serous?
|
visceral or epicardial
|
|
|
Cardiac tamponade is rapid filling of fluid with causing ________
|
restrictive diastolic filling
|
|
|
In A4, there is a dropout in the IAS -what might this be?
|
ASD
or normal dropout in that view |
|
|
Kids with Tuberous Sclerosis have what tumors?
|
rhabomyomas
|
|
|
Peripheral contrast is not useful in asd, ai, tr or vsd?
|
ai
|
|
|
Which view shows the coronary sinus in long axis?
|
A4 with posterior angulation
|
|
|
What is the valve of the IVC?
|
eustachian
|
|
|
What is meant by automaticity?
|
ability to initiate electric impulse
|
|
|
What does amyl nitrite to do HR?
|
increases
|
|
|
What is the difference between a pacer wire and a catheter?
|
pace wire goes to the apex. central lines stay in the atrium
swan ganz catheters usually do not go to the apex |
|
|
Why are right and left CA's called that?
|
because the left feeds the left side and the right the right
|
|
|
Why are the AV leaflets called what they are?
|
because the correllate to the CA's
|
|
|
Where does the LAD originate?
|
Anterior interventricular sulcus
|
|
|
A systolic rumble might be as, ms, ai, tr, or mr?
|
tr
|
|
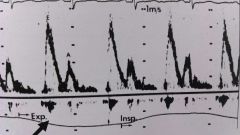
What is the arrow pointing to?
|
superimposed respiratory tracing
|
|
|
What do you do first for an apneic patient after giving sedation?
|
check airway
|
|
|
Why do IVC sniff test?
|
check for elevated RA pressure
|
|
|
What direction shunt causes cyanosis?
|
right to left
|
|
|
What is a pressure drop
|
same as a gradient across valves
|
|
|
In the cath lab, which formula is used for valve areas?
|
Gorlin
|
|
|
MV inflow velocity should not be affected by age, gender, HR, or preload
|
gender
|
|
|
Which valve is most likely to have regurg?
|
TV
|
|
|
What are four causes of acute MR?
|
endocarditis
ruptured chordae pap muscle dysfunct prosthetic valve dysfunct |
|
|
What what disease should you NOT rely on mmode for LV EF?
|
apical infarc
|
|
|
An MI of inferior wall involves which CA?
|
RCA
|
|
|
Which CA supplies LV apex?
|
lad
|
|
|
What percent of normals have PFO?
|
20-30%
|
|
|
What 2d finding would you see with PLSVC?
|
dilated coronary sinus
|
|
|
What causes pre-systolic opening of AV?
|
elevated LVEDP
|
|
|
Patients with ankylosing spondylitis may develop ms, as, mr, ar
|
ar
|
|
|
What is kyphosis?
|
exaggerated anterior spinal curvature
|
|
|
Why is it important to know cardiologically speaking?
|
because it can compress the PA causing PHTN
|
|
|
What is Uhls anomaly
|
congenital absent RV myocardium or parchment heart
|
|
|
What can Uhls's anomaly be confused with ?
|
Ebsteins
|
|
|
When can contrast dissipate too quickly low mi, high mi, low freq, high freq
|
high mi
|
|
|
Name three heart muscle layers
|
1. epicardium - thin outer layer
2. myocardium - mid wall (thickest) 3. endocardium - inside |
|
|
What is the normal amount of pericardial fluid
|
40 cc
|
|
|
All of the following may cause jugular distension except
1.tamponade 2. PHTN 3. TS 4. hpovolemia 5. constrictive pericarditis |
hypovolemia
|
|
|
What is ventricle is most likely to be affected by cor pulmonale and how
|
rv enlarges
|
|
|
How many weeks before fetal heart develops
|
6
|
|
|
enlarged heart on chest xray could be all of the following except
a. pericardial effusion b. pleural effusion c. as d. hypertrophic cardiomyopathy |
pleural effusion
|
|
|
Which embryonic aortic arch develops into the transverse arch
|
fourth
|
|
|
What is persistent fetal circulation
|
phtn with right to left shunting across pfo and pda
|
|
|
Are right-sided pressures elevated with valsalva
|
during strain phase - no
during release - yes |
|
|
What kind of murmur with vsd
|
harsh holosystolic
|
|
|
Which clinical finding is associated with friction rub
|
pericardial effusion
|
|
|
AR starts at beginning/end of IVCT/IVRT
|
beginning of IVRT
|
|
|
BiPlane Simpson rule is used for calculating
|
ef
|
|
|
What causes a left parasternal friction rub
|
pericarditis
|
|
|
In a4, where might you see reverberation artifact
|
apex
|
|
|
Is QRS depolarization or repolarization
|
depolarization
|
|
|
Where are most fibroelastomas
|
on valves
|
|
|
fibroelastomas are described as
|
frond like
|
|
|
What might you see with scleroderma
|
phtn or pericardial effusion
|
|
|
On mmode, which things may be confused with pericardial effusion (3)
|
DAO
calcified mitral annulus ascites |
|
|
How many years should echos be kept
|
7
|
|
|
Will an ascending ao dissection cause mr
|
no not severe maybe mild
|