![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
97 Cards in this Set
- Front
- Back
|
What does SSRI stand for? |
Selective Serotonin Reuptake Inhibitor |
|
|
What are the prototype SSRIs? |
1) Escitalopram 2) Fluoxetine 3) Sertraline |
|
|
What does SNRI stand for? |
Serotonin-Norepinephrine Reuptake Inhibitor |
|
|
What are the prototype SNRIs? |
1) Duloxetine 2) Venlafaxine |
|
|
What are the prototype atypical antidepressants? |
1) Bupropion 2) Mirtazapine |
|
|
What are the prototype tricyclic antidepressants? |
1) Amitriptyline 2) Nortriptyline |
|
|
Unless specified otherwise, all of the prototype antidepressant drugs are only available as _________ dosage forms. |
oral |
|
|
What two general categories are drugs used to treat mood disorders grouped into, and what are each of those groups principally used to treat? |
1) antidepressants - major depressive disorder 2) mood stabilizers - bipolar disorder |
|
|
Antidepressants have numerous additional indications, such as what? |
-anxiety -neuropathic pain |
|
|
What has driven the development of all current antidepressants? |
the monoamine hypothesis |
|
|
What are major depressive disorders associated with? |
diminished serotoninergic, adrenergic, and/or dopaminergic neurotransmission in the CNS |
|
|
What does the monoamine hypothesis predict? |
that drugs that enhance CNS monoaminergic neurotransmission in the CNS will alleviate depression |
|
|
What is the general effect of SSRIs on monoamines? |
increases serotonin (5-HT) |
|
|
What is the general effect of SNRIs on monoamines?
|
increases 5-HT and increases norepinephrine |
|
|
What is the general effect of atypical antidepressants on monoamines? |
individualized effects on 5-HT, norepinephrine, or dopamine signaling |
|
|
What is the general effect of tricyclic antidepressants on monoamines?
|
increases 5-HT and increases norepinephrine |
|
|
What is the general effect of monoamine oxidase inhibitors on monoamines?
|
increases 5-HT and increases norepinephrine
|
|
|
The onset of antidepressant effects takes several weeks, indicating what? |
that their actions are more complicated than simply correcting synaptic neurotransmitter levels |
|
|
What is the range of antidepressant classes, from most specific to least specific? |
1. SSRIs (most specific) 2. SNRIs 3. atypical antidepressants 4. tricyclic antidepressants (least specific) |
|
|
The incidence and variety of adverse effects generally increase with... |
non-specificity. |
|
|
What does drug selection often depend on? |
patient history and tolerance for specific adverse effects |
|
|
What can patient tolerance be enhanced by? |
lower initial dosages followed by gradual increases |
|
|
In general, what is the difference in efficacy of most antidepressants? |
small and inconsistent |
|
|
Rational drug selection often puts much emphasis on what? |
adverse effects and drug interactions |
|
|
What are the phases for the time course of drug treatment of major depression? |
1) acute phase treatment -an adequate acute drug trial often lasts 6 weeks 2) continuation phase treatment 3) maintenance treatment |
|
|
What is the preferred goal of acute therapy? |
complete subsidence of symptoms - remission (rather than an intermediate therapeutic response) |
|
|
What are the goals of the continuation and maintenance phases of therapy? |
the prevent the return of symptoms (prevent "relapse" or "recurrence") |
|
|
Why do patients often try multiple drugs? |
their response to specific drugs is difficult to predict |
|
|
Patients who fail to have an adequate response after multiple therapeutic interventions are said to have what? |
"treatment-resistant" or "treatment-refractory" depression |
|
|
What are mono therapy options for treatment-resistant depression? |
1. increase the dose of the current antidepressant 2. switch to a different antidepressant in the same drug class 3. switch to another antidepressant in a different drug class |
|
|
What are the combination drug therapy options for treatment-resistant depression? |
1. careful use of antidepressants from two different drug classes 2. addition of an "augmenting" drug to the current antidepressant |
|
|
What is the augmenting drug? |
NOT another antidepressant; a separate drug that has been established to enhance the therapeutic effects of antidepressants |
|
|
What are many augmenting drugs known to increase? |
the synthesis/release of monoamines |
|
|
What are three augmentation drug options and things to keep in mind about each? |
1) atypical antidepressants -currently being heavily promoted -more expensive -significant adverse effects 2) lithium -significant risk of adverse effects and toxicity 3) triiodothyronine |
|
|
What are the FDA-approved indications for Escitalopram? |
1) Major Depressive Disorder 2) Generalized Anxiety Disorder |
|
|
What are the FDA-approved indications for Fluoxetine?
|
1) Major Depressive Disorder 2) OCD 3) Panic Disorder 4) Bulimia |
|
|
What are the FDA-approved indications for Sertraline? |
1) Major Depressive Disorder 2) OCD 3) Panic Disorder 4) Social Anxiety Disorder 5) Premenstrual Dysphoric Disorder |
|
|
2 things to know about the use of SSRIs in depression |
1) often the drugs of choice, mostly for their lower incidence of serious adverse effects 2) there is a long delay (weeks) for antidepressant effects to occur |
|
|
In general, what is affected by SSRIs? |
several transporters & receptors in central serotoninergic neurons |
|
|
What is the main target of SSRIs? (main SSRI receptor) |
SERT, the presynaptic transporter which removes 5-HT from the synaptic cleft (SERT inhibition = increased synaptic 5-HT levels) |
|
|
What are the additional targets of SSRIs? |
various presynaptic & postsynaptic 5HT receptors that are directly or indirectly affected by SSRIs, enhancing serotonergic neurotransmission |
|
|
What is the most diverse NT receptor family? |
serotonin receptors |
|
|
What are the 5-HT receptor families and subtypes and their most common signaling pathways? |
1) 5HT1 (A-F) - inhibitor GPCR, decreases cAMP 2) 5HT2 (A-C) - excitatory GPCR, stimulates phospholipase C 3) 5HT7 - excitatory GPCR, increases cAMP |
|
|
relevance of 5HT1 and 5HT2 activation to SSRI effects |
contributes to both therapeutic & adverse effects |
|
|
relevance of 5HT7 activation to SSRI effects
|
activation may contribute to therapeutic effects |
|
|
Most 5HT receptors are (post or presynaptic?) and (inhibitory or excitatory?). |
-postsynaptic -can be either |
|
|
Presynaptic and somatodendritic (auto) receptors are excitatory or inhibitory? |
inhibitory |
|
|
What does the slow onset of beneficial effects for SSRIs suggest? |
a more complex mechanism of action than simply correcting synaptic NT levels |
|
|
What has the delayed therapeutic effect of SSRIs been hypothesized to be due to? |
additional mechanisms, including slower effects on neuronal viability, neurogenesis, and plasticity -ex) may promote dendritic arborization of hippocampal pyramidal neurons |
|
|
What might link SSRI effects on serotonin to slower neuronal changes? |
the neurotrophin BDNF |
|
|
mechanism of BDNF involvement |
(1) SSRIsinhibit SERT, which (2) elevates5-HT inthe synaptic cleft. (3)Activation of post-synaptic 5HT7 receptors (4)activates CREB (a transcription factor). (5) CREBincreases expression and release of BDNF (Brain-Derived NeurotrophicFactor). (6) BDNFreceptors (TrkB) promote neuronal growth, & neuroplasticity innearby neurons. |
|
|
In regards to the effects of SSRIs: Rapid enhancement of serotonergic neurotransmission likely causes...
|
most rapid onset adverse effects (ex: GI distress) |
|
|
In regards to the effects of SSRIs: Enhanced neuroplasticity may contribute to... |
the delayed onset of therapeutic effects |
|
|
What is the most specific SSRI? |
Escitalopram |
|
|
In addition to being an SSRI, Sertraline is also what? What is the significance of this? |
-a weak inhibitor of dopamine reuptake -The weak enhancementof dopamine neurotransmissionis modestlyactivating (stimulating) to some patients. May be desirable for hypersomnia, undesirable for insomnia. |
|
|
In addition to being an SSRI, Fluoxetine also does what? What is the significance of this?
|
-blocks norepinephrine reuptake and 5HT2C receptors -enhanced norepinephrine neurotransmission is also ananti-depressant mechanism |
|
|
Describe the withdrawal syndrome associated with some SSRIs. How do you avoid it? |
-uncomfortable, usually not dangerous -GI symptoms, irritability, paresthesias -avoid by tapering dose over 2-3 weeks |
|
|
What SSRI has a very long-lived active metabolite and may cause fewer withdrawal problems? |
Fluoxetine |
|
|
Some SSRIs are potent inhibitors of ____, and are prone to drug interactions. Which cause the least trouble? Which cause the most? |
-CP450 -Escitalopram -Fluoxetine, Sertraline |
|
|
What can cause "serotonin syndrome? |
combiningdrugs that either:
1) cause excessive 5HT release 2) directly activate5HT receptors 3) increase blood levels of serotonergic drugs |
|
|
early symptoms of serotonin syndrome |
-Neuromuscular problems(tremor,hyper-reflexia)
-Cognition & behavioral problems(incoordination, agitation) -Temperature control (fever, diaphoresis) |
|
|
late symptoms of serotonin syndrome |
tonic-clonic convulsions, organ failure |
|
|
drugs that can contribute to serotonin syndrome |
many SSRIs, SNRIs, TCAs, MAOIs (basically any antidepressant that elevates 5HT levels) |
|
|
common adverse effects of SSRIs |
1. nausea, GI cramping -prominent, but often transient upon starting drug therapy 2. "activating", insomnia -Moderate. More common with some SSRIs (e.g.fluoxetine). 3. anorgasmia, decreased libido -Prominent & more lasting effects. Often causes discontinuation. 4. anti-platelet effect Some increasedincidence of GI bleeding & stroke.Due todepletion of platelet serotonin. |
|
|
SSRIs are often used cautiously in what groups of people? |
during pregnancy and nursing ➤Little evidence of major teratogenicity, except for paroxetine(ventricular septal defects). ➤Some increased risk of neonatal pulmonary hypertension. |
|
|
What syndrome can occur in neonates that is associated with SSRIs? |
Postnatal Adaption Syndrome (SSRI withdrawal syndrome in neonates) |
|
|
In what groups of people is antidepressant use controversial? Why? |
adolescents and young adults ➤In 2004, FDAmandated a “black box” warning linking all antidepressants and suicidality. Warning has now been extended to anyone< 24 years old. |
|
|
Why has expert opinion been divided on whether SSRIs can increase suicidality? |
SSRI use may just be more likely in such patients |
|
|
What are the FDA-approved indications for Duloxetine?
|
1) Major Depressive Disorder 2) Fibromyalgia 3) Generalized Anxiety Disorder* 4) DiabeticNeuropathy* 5) ChronicMusculoskeletal Pain* |
|
|
What are the FDA-approved indications for Venlafaxine?
|
Major Depressive Disorder |
|
|
What do both Duloxetine and Venlafaxine block? |
both neuronal serotonin and norepinephrine uptake |
|
|
What is different about the blocking effects of Velafaxine (vs. Duloxetine)? |
Norepinephrinereuptake inhibition is weaker with venlafaxine. Behaves like an SSRI at low doses.
|
|
|
comparison of TCAs, SSRIs, and SNRIs |
-Older antidepressants(TCAs) affect multiple targets, causing many adverse effects.
-SSRIs (more specific)have fewer adverse effects, but lack some beneficial effects of TCAs. -SNRIs were developedas an intermediate between SSRIs & TCAs. |
|
|
What is the most important example of the fact that SNRIs have somewhat broader clinical uses than SSRIs? |
SNRIs are more widely used in chronic pain disorders |
|
|
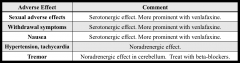
adverse effects of SNRIs (share most with SSRIs with some additions) |
|
|
|
How would you describe "atypical" antidepressants? |
a disparate drug group with individualized drug targets |
|
|
usage of Bupropion |
-commonly used antidepressant -also approved for seasonal affective disorder and nicotine withdrawal |
|
|
usage of Mirtazapine |
commonly used antidepressant |
|
|
Bupropion has unique properties, which may be due to what? |
possiblydue to combining inhibition of norepinephrine reuptake (NRI) with inhibition of dopamine reuptake (DRI)
|
|
|
Why can Bupropion be on of the safer drugs to include in antidepressant combinations? |
it will not contribute to excessive activation ofserotonergic systems
|
|
|
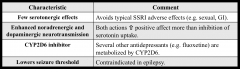
characteristics of Bupropion |
|
|
|
What makes Mirtazapine a valuable alternative to SSRIs? |
good efficacy and a different adverse effect profile (very effective anti-depressant, has unique advantages/disadvantages) |
|
|
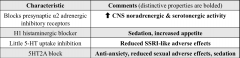
characteristics of Mirtazapine |
|
|
|
How is nortriptyline related to amitriptyline? |
The secondary aminenortriptyline is an active metabolite of the tertiary amine amitriptyline.
|
|
|
What are the FDA-approved uses of amitriptyline and nortriptyline? |
depression |
|
|
specificity of TCAs |
much less specific drugs than other antidepressant classes |
|
|
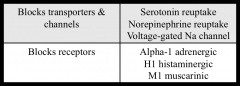
What things do TCAs block? |
|
|
|
What do TCA's multiple actions give them? |
both more varied clinical uses and more adverse effects |
|
|
What is the main mechanism of action for TCAs in depression? |
inhibiting serotonin & norepinephrine uptake (like SNRIs) |
|
|
What is the difference in secondary vs. tertiary amines in relation to NE and 5-HT? |
Secondary aminesaffect NE somewhat more than 5-HT.Tertiary amines aremore balanced.
|
|
|
How does the clinical efficacy of most TCAs in depression compare? |
all fairly similar |
|
|
Why are TCAs less commonly used in depression than SSRIs, SNRIs, or atypicals? |
adverse effects |
|
|
TCAs have many other (mostlyoff-label) uses than other antidepressant classes. They are often a drug of choice in what situations?
|
specific types of neuropathic pain (ex: diabetic neuropathy) |
|
|
Why is overdosage more dangerous with TCAs than other antidepressants? |
sodium channel block |
|
|
How can TCAs cause death from OD? |
-Initial excitatoryphase (seizures, agitation)
-Subsequent depressantphase (coma, depressed respiration) -A variety of cardiacarrhythmias may be induced. |
|
|
How do you prevent suicide in depressed patients while still administering necessary meds? |
-prevent accumulation of pills -get supervision help from family |
|
|
What types of problems can TCAs cause and what are the causes of these problems? |
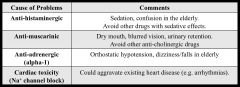
|