![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
73 Cards in this Set
- Front
- Back
|
Aerobic Gram (+) cocci |
Streptococci -pneumococcus -viridians -group A Enterococci Staphylococci -aureus -epidermidis |
|
|
Anaerobic Gram (+) rods |
Clostridia -difficile -tetani (C. diff overgrowth --> pseudomembranous colitis with clindamycin/ciprofloxicin) |
|
|
Aerobic Gram (-) rods |
Pseudomonas - easily fatal, resistant, nosocomial Helicobacter - PUD (duodenal, gastric = NSAIDs) E. coli - UTIs Klebsiella -UTI, pneumonia |
|
|
CNS infections (meningitis) are normally gram (?) |
(+) |
|
|
Anaerobic Gram (-) rods |
Bacteroides |
|
|
β-Lactams |
1. Bactericidal 2. Work on bacterial cell wall --> Inhibit the synthesis of the cell wall 3. Time dependent pharmacodynamics (need more frequent doses) |
|
|
β-Lactams Penicillins |
1. Penicillin 2. Ampicillin 3. Amoxicillin 4. Nafcillin 5. Amox-clavulanate |
|
|
β-Lactams Penicillins MSSA coverage |
Penicillin/Ampicillin = + Nafcillin/Amoxi-clav = ++++ Piperacillin-tazo = ++++ (hospital) |
|
|
β-Lactams Penicillins Streptococcal (nonpneumococcal) coverage |
Penicillin, Ampicillin, Amoxi-clav, Nafcillin ALL are ++++ This grip is very important for dentists |
|
|
β-Lactams Penicillins Enterococcal coverage |
Penicillin, Ampicillin, Amoxi-clav = ++ Nafcillin = NO coverage |
|
|
β-Lactams Penicillins E.coli (non ESBL+) coverage |
Ampicillin = ++ Amoxi-clav = +++ Piperacillin-tazo = ++++ |
|
|
β-Lactams Penicillins Klebsiella coverage |
Amoxi-clav = ++ Piperacillin-tazo = ++++ Ampicillin = NO coverage |
|
|
β-Lactams Penicillins Pseudomonal coverage |
Ampicillin, Amoxi-clav = NO coverage Piperacillin-tazo = ++++ |
|
|
β-Lactams Penicillins Anaerobic coverage |
Penicillin, Ampicillin = ++ Piperacillin tazo, Amoxi-clav = ++++ |
|
|
β-Lactams Penicillins ADRs |
Allergic type 1 hypersensitivity Diarrhea (ampicilllin, amoxi-clav) Nephritis Ampicillin rash (histamine release, not allergic) |
|
|
β-Lactams Cephalosporins 1st generation |
Cefazolin Cephalexin |
|
|
β-Lactams Cephalosporins 2nd generation |
Cefuroxime |
|
|
β-Lactams Cephalosporins 3rd generation |
Cefixime Ceftizoxime Cefdinir |
|
|
β-Lactams Cephalosporins 4th generation |
Cefepime |
|
|
β-Lactams Cephalosporins 5th generation |
Ceftaroline (the ONLY β-Lactam which covers MRSA) |
|
|
β-Lactams Cephalosporins Staph. aureus (non-MRSA) coverage |
Cephalexin, Cefazolin, Cefuroxime = ++++ |
|
|
β-Lactams Cephalosporins Streptococci (non-pneumococcal) coverage |
Cefazolin, Cephalexin, Cefuroxime, Cefepime ALL are ++++ |
|
|
β-Lactams Cephalosporins Pneumococcal coverage |
NOT that great (we aren't really worried about) Cefexime, Ceftriaxone = +++ |
|
|
β-Lactams Cephalsoporins E.coli (non ESBL+) coverage |
Cefazolin, Cephalexin, Cetriaxone = +++ Ceftazidime = ++++ |
|
|
β-Lactams Cephalosporins Pseudomonal coverage |
Cefepime, Ceftazidime = ++++ Cefazolin, Cefuroxime = NO coverage |
|
|
β-Lactams Cephalosporins MRSA coverage |
Ceftaroline (ONLY) |
|
|
β-Lactams Cephalosporins ADRs |
Cross-reactivity with penicillins (low chance, 6-8%, even lower in higher gens) |
|
|
β-Lactams Carbapenems Drug(s), indications |
Imipenem, Meropenem, Doripenem Very Broad Spectrum Used for very severe nosocomial infections See slide 26 for efficacy (good except no MRSA) |
|
|
Drug Allergy Criteria |
1. Rxn occurs in small # of pts 2. Rxn does NOT resemble pharm effects 3. Rxn occurs even with small amt of drug 4. Rxn occurs in drugs w/ similar structure 5. Presence of eosinophilia 6. Rxn resolves on discontinuation |
|
|
Cross-Reactivity PCN allergy info |
10-20% pt report PCN allergy (BUT 80-90% negative skin test) -- Ask Q's Less than 10% cross-reactivity between PCNs and Cephalosporins in gen pop. |
|
|
True Allergic Reaction Symptoms |
Skin rash, hives, difficulty breathing (wheezing), dizziness and hypotension (severe) Hypotension due to histamine release, PG and Leukotrienes |
|
|
Macrolides Drug(s) & MOA |
Azithromycine, Clarithromycin, Erythromycin Binds to 50s Ribosomal subunit --> inhibit protein synthesis |
|
|
Macrolides Coverage Gram (+): MSSA, MRSA, Strep (np), Entercocci, pneumococci |
MSSA = ++ MRSA = NONE Streptococci (non pneumococcal) +++ Enterococci = NONE Pneumococci = ++ |
|
|
Macrolides Coverage Gram (-), Anaerobes |
Minimal Gram (-), NO anaerobic coverage |
|
|
Quninolones Drugs(s), MOA, Bacterio________, pharmacodynamics |
Ciprofloxacin, Levofloxacin, Moxifloxacin & Gemifloxacin Cause DNA breakage Bactericidal Concentration dependent pharmacodynamics (only need one big dose vs. β-Lactams) |
|
|
Vancomycin MOA, spectrum, Dosage form |
Inhibits Gram (+) cell wall synthesis Broad Gram (+) coverage, including MRSA IV only, except PO for C. diff colitis (no abs needed) |
|
|
Vancomycin ADRs |
Nephrotoxicity (dose and duration) Redman syndrome (related to infusion time) Phlebitis (concentration) |
|
|
Clindamycin Class, MOA, ADR |
Lincosamide Binds to 50s ribosomal subunit --> inhibits protein synthesis May cause pseudomembranous colitis (C. diff overgrowth) |
|
|
Clindamycin Coverage Gram (+): Enterococci, MRSA, Strep (np), MSSA Gram (-), Anaerobes |
Enterococci __, MRSA +, Streptococci, +++, MSSA ++++ No Gram (-) coverage Anaerobic coverage +++ |
|
|
Trimetoprim-sulfomethoxazole Pt population? |
Seen in post-transplant pts prophylaxis |
|
|
Trimetoprim-sulfomethoxazole ADRs |
Photosensitivity (big one!) Rash (rarely SJS) Hyperkalemia, Neutropenia, Thrombocytopenia, Cholestasis GI (N/D) |
|
|
Tetracyclines Drug(s), coverage |
Doxycycline, Minocycline, Tigecycline (mp) Gram (+) +++ (including MRSA, VRE) Gram (-) +++ Anaerobic +++ NO Pseudomonas coverage |
|
|
Tetracyclines ADRs |
Allergic rxn Photosensivity GI (N/V) Tooth discoloration in children |
|
|
Infective endocarditis |
An infection of heart chambers or valves (Vegetation = hallmark) |
|
|
ABX Prophylaxis against Endocarditis Cardiac conditions w/ high risk of IE |
1. Prosthetic cardiac valve 2. Prosthetic material for cardiac-valve repair 3. Previous hx of IE 4. Congenital Heart dz (CHD) (unrepaired, repaired within 6 months, repaired with residual defects) 5. Cardiac transplant recipients with valvulopathy |
|
|
ABX Prophylaxis against Endocarditis Prophylaxis NOT required |
1. Mitral valve prolapse 2. Rheumatic heart disease 3. Bicuspid valve disease 4. Calcified aortic stenosis 5. CHD: VSD, ASD, hyptertrophic cardiomyopathy |
|
|
ABX Prophylaxis against Endocarditis Dental treatments requiring prophylaxis |
All dental procedures involving manipulation of gingival tissue or the PA region of teeth or perforation of oral mucosa Extraction, routine cleaning, SRP, RCT, orthodontic bands, sub gingival medications, biopsy, suture removal |
|
|
ABX Prophylaxis against Endocarditis Prophylactic Regimin |
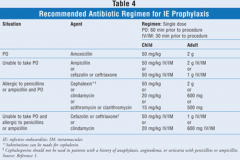
see slide 52 |
|
|
Advantage of Minocycline Subgingival ABX insertion |
Localized, therefore, no systemic toxicity and less resistance Better pt compliance |
|
|
Chlorhexidine Gluconate Uses |
Antibacterial dental/oral rinse Periodontal pocket chip |
|
|
Chlorhexidine Gluconate Coverage |
Covers gram (+), gram (-) and anaerobic bacteria |
|
|
Chlorhexidine Gluconate ADRs |
With long term use, causes discoloration of restorations, which may be permanent May cause oral mucosal irritation |
|
|
Chlorhexidine Gluconate Rinse, directions |
15 ml of 0.12% solution rinsed and expectorated for 30 seconds BID
|
|
|
Chlorhexidine Gluconate Periodontal chip |
Up to 8 chips per visit, no need for removal If dislodgment happens after 7 days, the tx is complete IF dislodgment happens within 1st 48 hrs --> needs reinsertion |
|
|
Amphotericin B, (IV) Class, Coverage |
Broad spectrum fungicidal agent Covers Candida and Aspergillus |
|
|
Amphotericin B, (IV) ADRs |
Nephrotoxcity Hypo Mg Hypo K |
|
|
Amphotericin B, (IV) Infusion related ADRs How to avoid? |
Rigor, hypotension, fever, nausea Premedicate with meperidine, hydrocortisone, acetaminophen, diphenhydramine, respectively. |
|
|
"Azole" Antifungals Drug(s) |
Itraconazole (PO) Fluconazole (PO/IV) Ketoconazole (PO/topical) Voriconazole (PO/IV) Posaconazole (PO/IV) |
|
|
Fluconazole (PO/IV) |
Candida infections |
|
|
Ketoconazole (PO/topical) |
Mostly used as an ANTI-ANDROGENIC agent Topical antifungal uses |
|
|
Voriconazole (PO/IV) |
Broad spectrum ADRs: visual changes, photophobia |
|
|
"Azole" antifungals CYP activity |
All "azoles" are CYP 450 INHIBITORS Many drug interactions Electrolyte imbalance --> Hypokalemia Can lead to increase risk of bleeding |
|
|
Oropharyngeal Candidiasis Treatment Options |
Clotrimazole troches (10mg) desolved swollen mouth 5x/day for 7-14 days Nystatin 500,000 units suspension swish --> spit/swallow 4x/day for 7-14 days Fluconazole 100-200mg PO 1x/day for 7-14 days |
|
|
Herpes Simplex Labialis (Cold sores/fever blisters) |
-HSV-1 primarily labial infection -HSV can be latent and reactivated -HSV is contagious and transmitted through direct contact (kissing, sharing utensils, etc) -Virus is also viable on the surface of objects for few hours -HSV enters host though skin/mucous membrane and becomes latent in trigeminal ganglia |
|
|
Herpes Simplex Labialis Triggers |
Ultraviolet radiation Stress Cold Fatigue Any factor that depresses the immune system |
|
|
Herpes Simplex Labialis When should it be treated? |
Prodromal phase with tingling, burning sensation |
|
|
Herpes Simplex Labialis Pharmacological treatment |
Benzocaine Dibucaine Benzyl alcohol Camphor Skin protectant to keep surface from dryness |
|
|
Herpes Simplex Labialis Pharmacological treatment (OTC) |
Docosanol 10% The only FDA approved OTC Must apply soon in prodromal 5x/day application IF secondary infection, use triple bio ointment (not directly over the other) |
|
|
Herpes Simplex Labialis Pharmacological considerations |
Avoid topical/systemic steroids NSAIDs and acetaphinophen may be used for pain relief |
|
|
Pharmacological treatment Natural supplements |
Tea tree oil (proven anti-viral) |
|
|
Halitosis |
Oral malodor/bad breath 90% are due to poor OH --> dental caries, gingival infection, tongue coating, impacted food, mucosal irritation, xerostomia |
|
|
Halitosis Nonpharmacological care |
Most bad breath is due to Volatile Sulfur Compounds (VSCs) after the break down of food debris by bacteria Prevent by removal of plaque-->caries Brushing/Flossing/Tongue blade |
|
|
Halitosis Pharmacological care |
Zinc Salts and chlorine dioxide (antibacterial, prevent VSC production by inhibiting metabolism to form sulfur compounds) "Smart Mouth" combines them both "CloSYS" does not |