Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
52 Cards in this Set
- Front
- Back
|
boundaries of the abdominopelvic cavity and its subdivision into abdominal & pelvic cavities
|
Abdominal cavity - bounded by:
- diaphragm (roof) - anterolateral abdominal wall - posterior abdominal wall - pelvic inlet (opening between abdominal cavity & pelvic cavity) |
|
|
anterolateral abdominal wall and the nerves that supply it
|
T7-11 (intercostal nn.)
T12 (subcostal n) L1 (illioinguinal + illiohypogastric nn) |
|
|
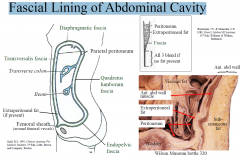
name the layers penetrated by a needle passed into the peritoneal cavity through the midline of anterior abdominal wall
|

•Skin
•Superficial fascia •Deep fascia (very thin) •Linea alba •Transversalis fascia •Extraperitoneal fat •Parietal peritoneum |
|
|
Neddle through the lateral Abd Wall
|
•Skin
•Superficial fascia •Deep fascia (very thin) •External oblique •Internal oblique •Transversus abdominis •Transversalis fascia •Extraperitoneal fat •Parietal peritoneum |
|
|
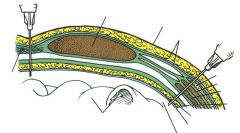
significance of the membranous layer of deep fascia (Scarpa’s fascia)
|
Clinical significance of membranous layer: It forms a self-contained pouch inferiorly that may fill with urine that extravasates from a ruptured urethra in males (arrows indicate path taken by urine in cases of ruptured urethra e.g., straddle injuries).
Sutures through membranous layer cosmetically better result (strengthens healing wound, reduces skin stretch). |
|
|
structures that converge on the internal aspect of the umbilicus and how they relate to early development
|
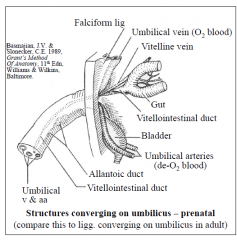
- all layers fuse at umbilicus
- • ~LV3/4 level (but variable) • site of attachment of umbilical cord • a consolidated scar • all layers of ant. abdominal wall fused here • may evert with raised intraabdominal pressure (e.g., ascites or large mass (tumour, foetus) • abdominal aorta bifurcates about 1cm below and to left |
|
|
muscles of the anterior abdominal walls and state their actions
|
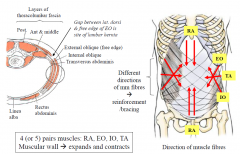
- mm contract to move trunk (flex, rotate & laterally flex the trunk)
- mm contract during forced expiration (pull ribs down, compress abd viscera & force a relaxed diaphragm upward) - mm contract to compress abdominal viscera & increase intra-abdominal pressure (diaphragm also contracts) e.g., lift, strain, expel abdominal contents (vomit, defaecate, childbirth), prior to cough or sneeze - reflex contraction to protect viscera against injury (“guarding”) e.g., generalised peritonitis board-like rigidity - resting muscle tone support of viscera (loss of muscle tone locally eg nerve damage visceroptosis) |
|
|
formation of the rectus sheath
|
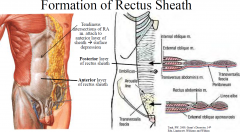
FUNCTION: retains rectus abdominis muscle and provides added support to the ant abdominal wall
Above arcuate line: ant. layer is formed by aponeurosis of EO & ant part of aponeurosis of IO, post. layer is formed by post part of IO aponeurosis & all of TA aponeurosis Below arcuate line: ant. layer is formed by all 3 aponeuroses of EO, IO and TA; post. rectus sheath is absent - rectus abdominis muscle is in contact with transversalis fascia |
|
|
significance of enlarged superficial veins on the anterior abdominal wall
|
- can signify liver failure (patent paraumbicialc v.) from portal backflow
|
|
|
lymphatic drainage of skin & superficial fascia of trunk wall above and below the umbilicus/iliac crest
|
- below to inguinal
- above to axillary |
|
|
Abdominal Wall:
functions |
1. expansile
accommodate considerable changes in volume 2. contractile support of contained viscera (resting tone of mm) move the trunk (eg, rotation, flexion) increase the intra-abdominal pressure (eg, straining, or prior to cough /sneeze) |
|
|
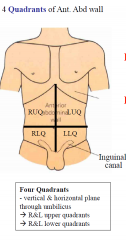
Quadrants of Ant Abd Wall
|
|
|
|
Regions of the Ant Abd Wall
|

|
|
|
Camper's Fascia
|
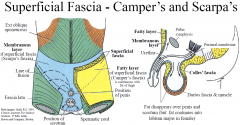
fatty layer superficial fasica
- continous with the thigh |
|
|
Scrapas Fascia
|
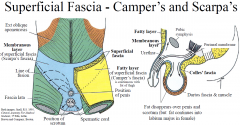
membranous layer of superficial fascia
- ends 1cm below the inguinal ligament where it fuses with deep fascia of the thigh - It extends into the perineum and is continuous with (dartos) fascia around penis and scrotum and attaches to ischiopubic ramus and posterior edge of perineal membrane. |
|
|
External Oblique
|
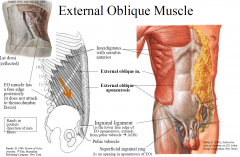
Attachments: Lower 8 ribs (ext surface) linea alba, pubic tubercle, ant ½ iliac crest, inguinal ligament
Action: trunk flexion & contralateral rotation; compress abdominal viscera; Innervation: T7-T12 |
|
|
Internal Oblique
|
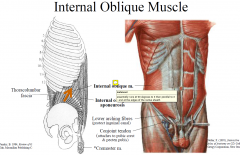
Attachments: Thoracolumbar fascia, ant 2/3rd iliac crest, lat 2/3rd ing lig ribs 10-12, linea alba & pecten pubis via conjoint tendon
Action: trunk flexion, ipsilateral rotation, compress abdominal viscera, Innervation: T7-L1 (iliohypogastric & ilioinguinal nn) *Gives rise to cremaster muscle (skeletal muscle: contraction elevates testis) |
|
|
Transversus Abdominis Muscle
|
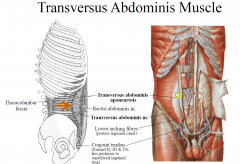
Attaches: Lower 6 ribs (int surface), thoracolumbar fascia, iliac crest, lat 1/3 ing lig linea alba & pecten pubis via conjoint tendon
Action: compress & support abdominal viscera, Innervation: T7-L1 (iliohypogastric &ilioinguinal nn) |
|
|
Rectus Abdominis Muscle
|
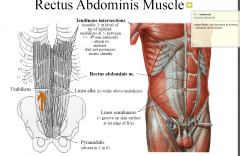
Attaches: Pubic symphysis and crest xiphoid process & cc 5-7
Action: trunk flexion, compress abdominal viscera, stabilise tilt of pelvis (antilordosis) Innervation: T6/7-12 |
|
|
Rectus Sheath Above and below arcuate line
|
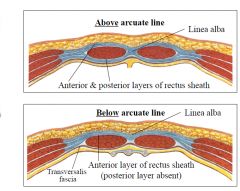
Above arcuate line, ant & post layers of rectus sheath are formed by 1 ½ aponeuroses each
Below arcuate line, all 3 aponeuroses pass anterior to rectus abdominis The superior and inferior epigastric vessels anastomose within the rectus sheath. If the aorta is occluded, collateral supply to the lower parts of body occurs through these arteries. they travel below rectus abdominis |
|
|
Linea alba
|
midline, tendinous raphe (from xiphoid to pubis); formed by aponeuroses of EO, IO & TA of both sides
- the area surgeons love; it does not bleed |
|
|
Fascial Lining of Abdominal Cavity
|
|
|
|
Peritoneal folds on internal aspect of anterior abdominal wall
|
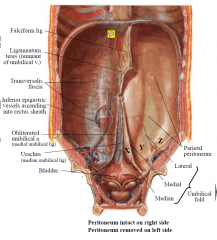
1. Falciform ligament, with ligamentum teres in its lower edge, ends at umbilicus.
2. Median, medial & lateral umbilical folds are ridges formed respectively by peritoneum over the urachus (abdominal remnant of allantois), L&R obliterated umbilical artery and L&R inferior epigastric vessels. The median and medial umbilical folds converge on the umbilicus. The lateral fold ascends towards rectus abdominis. - bleeding will occur if the lateral umbilical fold is cut |
|
|
Arterial Supply
|
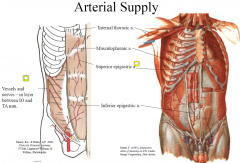
The superior and inferior epigastric vessels anastomose within the rectus sheath. If the aorta is occluded, collateral supply to the lower parts of body occur through the sup and inf epigastric aa.
|
|
|
Venous Supply
|
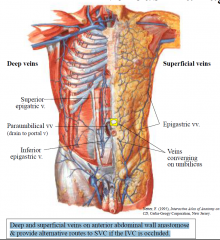
Deep and superficial veins on anterior abdominal wall anastomose & provide alternative routes to SVC if the IVC is occluded.
|
|
|
Prominent Superficial Veins
|

- paraumbilical vein is closed but can reopen in liver failure
|
|
|
LN in abd wall
|
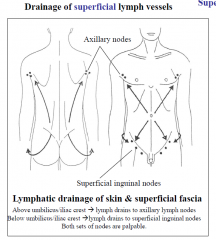
Superficial lymph vessels of abdominal wall drain the skin & superficial fascia (to axillary or superficial inguinal lymph nodes) Deep lymph vessels drain muscle & tissues deep to this and drain along arteries to nodes associated with these aa. (eg to lateral aortic, parasternal, external iliac, inguinal nodes)
|
|
|
Nerves
|
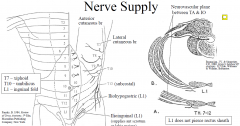
T7-T11(12) (thoracoabdominal = lower IC nn and subcostal n. (T12) that continue forward & down from IC spaces to abdominal wall L1 = iliohypogastric & ilioinguinal nn. Ilioinginal n. passes through inguinal canal.
|
|
|
Clinical Significance of nn
|
Significance: Irritation of lower 6 thoracic nn. can pain referral to abdominal wall; shingles of these nerves blisters and pain on thoracic & abd wall. Nerves innervate skin, muscle & parietal peritoneum therefore irritation of parietal peritoneum reflex mm. spasm, ie. “guarding” of abdominal wall (= attempt to rest and localise the inflammatory process). Generalised peritonitis board-like rigidity. Rebound tenderness occurs when inflamed parietal peritoneum is stretched - even when that movement is elicited by removing the hand from a distant site. Damage to nerves, e.g., abdominal incision paralysis of muscles (weak area, unsightly bulge & visceroptosis)
Avoid vertical incisions of lateral part of rectus muscle, which would sever its nerve supply weakness |
|
|
Abdominal Reflex
|

Abdominal reflex – stroke each quadrant of ant. abdominal wall reflex mm contraction (umbilicus drawn to side of contraction) – tests segmental nerves (also absent in some forms of brain damage e.g., stroke).
|
|
|
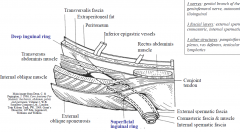
Inguinal Canal
|
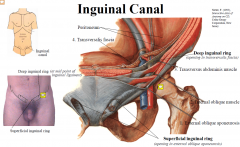
-
Oblique passageway through the muscles and fascia of the lower anterior abdominal wall - Located above the medial half of the inguinal ligament - From the deep to the superficial inguinal ring it is about 4cm long - Contains the spermatic cord (male) or the round ligament (female), and the ilioinguinal nerve |
|
|
Layers of the Inguinal Canal
|
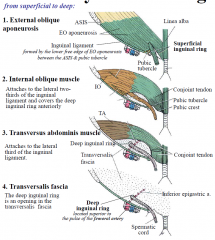
1. EO aponeurosis
2. IO muscle 3. TA muscle 4. transversalis fascia |
|
|
Boundaries of the inguinal canal
|
Floor Inguinal ligament
Roof Internal oblique and transversus abdominis muscles Anterior External oblique aponeurosis and internal oblique muscle Posterior Transversalis fascia and conjoint tendon |
|
|
The conjoint tendon
|
Formed from the lower part the transversus abdominis muscle
Inserts into the crest of the pubis and lies immediately behind the superficial inguinal ring Serves to protect an otherwise weak point in the abdominal wall |
|
|
Shutter-like effect of transversus abdominis and internal oblique
|
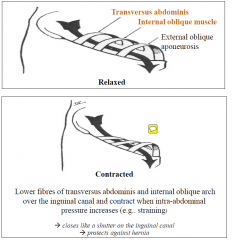
Transversus abdominis and internal oblique close like a shutter on the inguinal canal in response to increased intra-abdominal pressure, serving to protect against herniation.
|
|
|
Q.What is the relationship between a previous appendectomy and a right sided inguinal hernia?
|
A. The right ilioinguinal nerve (L1) may be damaged during an open appendectomy weakness of the shutter-effect of the arching fibres of transversus abdominis and internal oblique
|
|
|
Spermatic Cord:
Contents |
3 arteries: cremasteric, deferential artery, testicular
3 nerves: genital branch of the genitofemoral nerve, autonomic, ilioinguinal 3 fascial layers: external spermatic, cremasteric, internal spermatic 3 other structures: pampiniform plexus, vas deferens, testicular lymphatics |
|
|
Coverings of the spermatic cord and testes and their origns
|
Transversalis fascia internal spermatic fascia
Internal oblique muscle cremasteric fascia &muscle External oblique aponeurosis external spermatic fascia |
|
|
Anatomical location of deep inguinal ring
|
The deep inguinal ring is located superior to the pulse of the femoral artery
|
|
|
Conjoint tendon
|
The conjoint tendon is formed by the lower half of transversus abdominis and serves to protect an otherwise weak point in the abdominal wall. It lies behind the superficial inguinal ring.
|
|
|
Hernias
|
A hernia is a protrusion through a structure that normally contains it
|
|
|
Parts of a hernia
|
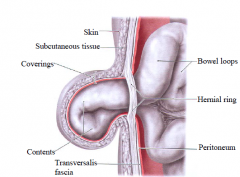
(1) Hernial sac Usually a pouch of peritoneum
(2) Contents Generally structures from the abdominal cavity e.g. fat, omentum or bowel (3) Coverings Contains layers from the abdominal wall through which the hernial sac passes |
|
|
2 types of hernias
|
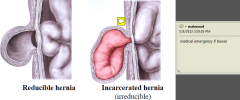
If the neck of the sac is narrow, adhesions & strangulation are common
|
|
|
Inguinal Hernias
|
|
|
|
Direct and Indirect Hernias
|
|
|
|
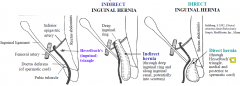
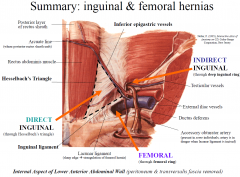
Hesselbach's Triangle bounded by
|
1. rectus abdominis
2. inferior epigastric a. 3. Inguinal ligament |
|
|
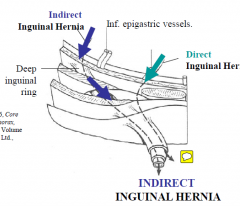
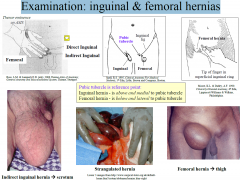
Indirect inguinal hernia
|
-passes through deep inguinal ring lateral to inferior epigastric artery
-most common type of inguinal hernia (2/3rd) -occurs in young & old -males > females; -may extend through superficial inguinal ring into scrotum -narrow neck (important in strangulations) |
|
|
Direct Inguinal Hernia
|
-passes through weakness in anterior abdominal wall via Hesselbach’s triangle medial to inferior epigastric artery
-through or around a weak conjoint tendon -age >40 years -less common than indirect hernia -rarely enters scrotum -wide neck of hernia (rarely strangulates) -lump at superficial inguinal ring |
|
|
Femoral Hernia
|
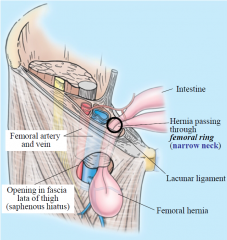
- Passes through femoral ring into thigh
- Protrudes through saphenous opening in fascia lata - More common in females than males (4:1) - Femoral ring forms neck of the hernia. Boundaries: - Inguinal ligament (anterior) - Pectineus muscle & fascia (posterior) - Femoral vein (lateral) - Lacunar ligament (medial) - Sharp margin of the lacunar ligament can cause strangulation of the hernia (surgical emergency) |
|
|
Summary Slide of Hernias
|
|
|
|
Examination: inguinal & femoral hernias
|
|
|
|
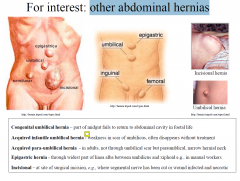
other abdominal hernias
|
|