![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
18 Cards in this Set
- Front
- Back
|
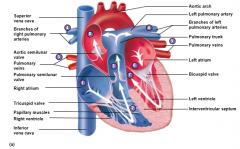
Parietal pericardium Visceral pericardium |
•Parietal pericardium: lines the fibrous outer layer •Visceral pericardium(epicardium): covers heart surface Cavitybetween two layers is filled with serous fliud, reduces friction |
|
|
•Pectinate muscles: •Trabeculae carnae: |
•Pectinate muscles:muscular ridges in auricles and right atrial wall •Trabeculae carnae:muscularridges and columns on inside walls of ventricles |
|
|
•Threelayers of tissue –Epicardium: –Myocardium: –Endocardium: |
•Three layers of tissue –Epicardium: Serous membrane; smooth outer surface of heart –Myocardium: Middle layer composed of cardiac muscle cell and responsibility for heart contracting –Endocardium: Smooth inner surface of heart chambers |
|
|
Atrioventricular valves(AV valves) Semilunar valves |
Atrioventricular valves (AV valves)-attachedto cone-shaped papillary muscles by tendons (chordae tendineae). Right has three cusps (tricuspid).Left has two cusps (bicuspid, mitral) Semilunar valves.Right (pulmonary); left (atrial). |
|
|
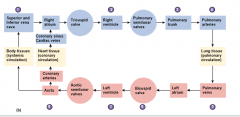
drop of blood traced through |
Bloodcomes from superior vena cava, infeferiorvena cava, or coronary sinus –> right atrium-> contracts, so tricuspid valve opens and allows blood to go the right ventricle-> pressure closes triscuspid vlave,then ventricle contracts, right semilunar valve opens, blood goes into pulmarytrunk, pressure causes semilunar canal to close, blood go to lungs and becomesoxygenated-> four pulmonary veins goes to left atrium, left atrium contracts pushing mitralvalve open, left ventricle fills, pressure raises so bicuspid valve closes,left ventricle contracts, left semilunar valve opens -> blood goes into aorta and slamssemi lunar canal |
|
|
|
|
|
SA node (the pacemaker) AV node Pirkinje fibers |
SAnode- happens in right atrium(alsocontracts with left atrium) then goes to AV nodeLocalspontaneous action potential – not from CNS, it stimulatesitself Influenced by parasympathetic andsympathetic system 100 Beats per minute with noinfluenceAverage 70 Beats per minute withparasympathetic influence Purkinje fibers- are muscle fibersthat are really good at conducting electricity (almost as good as neurons),slows it down so everything doesn’t happen too fast .11 seconds -> from SA to AV |
|

|
•Longrefractory period prevents tetanic contractions |
|
|
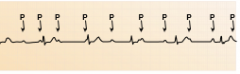
PQ interval QT interval QRS complex |
•PQ interval or PR interval:0.16 sec;atria contract and begin to relax, ventricles begin to contract • QT interval: 0.36 sec; ventricles contract and begin torelax •QRS complex: ventriculardepolarizationandsignals onset of ventricular contraction. Repolarization of atriasimultaneously. |
|
|
1)HeartBlock- When P wave and QRS complex are not coordinated. Somewhere betweenSA node to AV node there is a problem. |
|
|
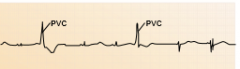
2)Premature ventricular contraction- no P wave proceeds the QRS complex |
|
|
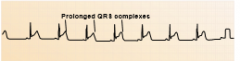
3) Bundle branch block- prolongedQRS complex- ventricle stays contracted too long |
|
|
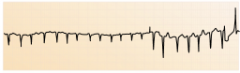
4)Atrial fibrillation – a fib – NoP waves and very rapid QRS complex, will gravity fill into ventricle |
|
|
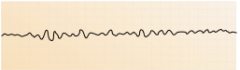
5)Ventricular fibrillation – No P,No QRS, No T- fluttering of ventricle |
|
|
Tachycardia Ventricular tachycardia atrial flutter |
tachycardia - heart race above 100 bpm Ventricular tachcardia- AV node probs, frequent fibrillation Atrial flutter- 2 or 3 P waves for every QRS |
|
|
atrial fibulation Bradycardia Premature Ventricular Contractions(PVCs) |
Atrial fibulation- no P waves Brady cardia- heart rate less than 60 bpm PVCS- prolonged QRS complex |
|
|
end diatstolic volume- Ejection fraction |
end diatstolic volume- ventricle is filled fully Ejection fraction= end diastolicvolume – end systolic volume |
|
|
Meanarterial pressure – about 98, would be 100 but spend alittle more time in restPre-load – left ventricle is allthe way filled and a bit stretched – frank-starling effect – the stretch on theheart greaterpreload increases stroke volume Afterload – almost empty, but justrunning out of blood, still pushing a bit |
Greater stroke volume thus greatercardiac output – means very small after load Contractility – feature in everymuscle, the more contractile, the greater degree it can contractEnd systolic volume will decreasewhen contractility increases Ionotropy– another word for contractility |