![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
96 Cards in this Set
- Front
- Back
|
Human Groups Studied in alcohol |
•Youth•UniversityStudents•Olderindividuals•Clinicalpopulations Øtraumaticbrain injury survivors and others with brain injury Øpeopletaking other drugsØchildrenand adults with FAS (Fetal Alcohol Syndrome)(Mostof these studies are non-experimental) |
|
|
How is alcohol made |
•Madeby ’fermentation’ØYeast(naturally occurring) converts sugar water to ethanol and CO2ØDrinkdetermined by source of sugar (grapes, grains, etc.)ØYeastsonly tolerate low levels of alcohol so fermentation à 10-15% acohol in solution |
|
|
Afterfermentation, distilling alcohol increasesalcohol content by how much? |
up to 40-50% usually |
|
|
Basic DistillationProcess |
ØBoil the solution (containing alcohol & water) Ø ØAlcohol boils first Ø ØSteam released by alcohol condenses Ø ØCondensation captured as a new liquid with a higher alcohol content than the original solution |
|
|
Earlydistillation |
– around 3000 BCE – probably in China |
|
|
Alcohol brewedsince about __________ (with advent of agriculture) |
6-8,000 BCE |
|
|
•Writtenguides to consumption appear about ____________ |
3,000-2,000 BCE |
|
|
•Platothought that young people should learn to drink so that they could learn to _____ _________ |
practice moderation |
|
|
•The decline of the Roman Empire is associated with what? |
excess consumption of alcohol (perhaps partially caused by lead poisoning from wine storage containers) |
|
|
•InEngland a consumption problem developed when? |
between 1684 and 1727 (~40 yrs) |
|
|
Temperance Movement in the US& development of a national Prohibition Party |
•1830-1860 |
|
|
•Prohibitionestablished in ______ and ended in ____ (during this time smuggling and illegalproduction were rampant – rapid development of organized crime) |
1917; 1933 |
|
|
•Steadyincrease in American consumption to ____ (decline since) |
1979 |
|
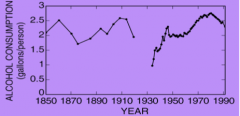
Whatis the important point demonstrated bythis graph? |
Yearlyalcohol consumption, in gallons per person, of raw alcohol from 1850 to 1990 inthe United States |
|
|
___ of young adults (15-24 yrs) reported usingalcohol in the previous 12 months (____ of individuals over 25) |
70%; 80% |
|
|
•Youngadults report starting to drink at ~_____ whereas older adults report usestarting at ~____ |
16yrs; 18yrs |
|
|
Canadian Guidelines for Consumption |
1.Set limits for yourself and stick to them. 2.Drink slowly. Have no more than 2 drinks in any 3 hours.3.For every drink of alcohol, have one non-alcoholicdrink. 4.Eat before and while you are drinking. 5.Always consider your age, body weight and healthproblems that might suggest lower limits. 6.While drinking may provide health benefits for certain groups ofpeople, do not start to drink or increase your drinking for health benefits. |
|
|
WHat does low risk drinkng help with? |
helps to promote a culture of moderation and supports healthy lifestyles. |
|
|
•BloodAlcohol Level (BAC) |
is concentration in the blood •Can be measured via the blood or breath |
|
|
How to measure Blood Alcohol Level (BAC) |
•Breathalyzermeasures breath but this is a reliable measure of BAC•Unitsof measure are mg/100ml (e.g., 80 mg/100 mlrepresents .08% alcohol in theblood) |
|
|
Ontario Laws – New “Warn Range” between |
.05 and .08 |
|
|
•Iwould not be “safe” to drive for at least 2 hours and I would still not be surebased on things like: |
ØAge (I’m in my 50s so I probably don’t metabolize as well as a younger person) ØHealth (I might have a head cold or maybe a chronic health condition) ØExperience with alcohol (I have very little metabolic tolerance because I rarely drink alcohol) Other drugs (say, an alcohol-containing cough medicine for my cold or even medicine for my heartburn after dinner) |
|
|
Administration and Absorption of alcohol |
•Oraladministration•Alcoholdoes not ionize – easily absorbed•First-passmetabolism (alcohol dehydrogenase) in the stomach•So,if food is present, this will keep alcohol in the stomach longer and morefirst-pass metabolism will occur•LowerBAC•BUT…. same peak |
|
|
True or False Alcohol does not ionize |
True |
|
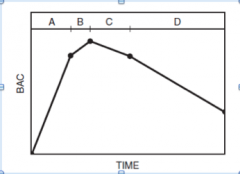
Pharmacokinetics of Alcohol |
Theoreticaltime course for BAL after taking a single drink.A:Absorption PhaseB& C: Plateau PhaseD:Excretion PhaseTimeto reach B is about an hourPeak15 mins laterTimeto B is reduced by 20 mins with additional drinks |
|
|
Factors Affecting Absorption |
•Stomachacidity medicines (e.g. cimetidine/Tagament & ranitidine/Zantac)ØH2-receptorantagonists ØReducelevels of alcohol dehydrogenaseØCanincrease absorption into blood by 17%ØGreatesteffect on a full stomach•SexdifferencesØFemaleshave lower levels of alcohol dehydrogenase in stomach•Beerpasses through stomach more slowly à less alcoholabsorbed•Carbonationfacilitates à more alcoholabsorbed •Higheralcohol content à increased diffusionrates (most rapid absorption at 40%)Expectancy à higher BACFactors Affecting Absorption |
|
|
Distribution |
•Doesnot dissolve in fat (women have more body fat)ØManand woman of same weight and who drink same weight à female will have higher BAC in body fluid (water) ØMalebody fat increases with age à so does BAC (thiseffect not observed for women)•Isevenly distributed in the body•Crossesblood-brain and placental barriers•So… can be measuredanywhere, including in exhaled vapours |
|
|
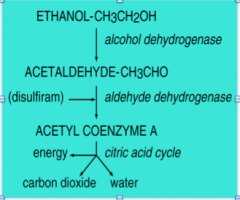
Elimination |
•90-98%eliminated by the liver (metabolized)•Efficientsystem•Two-stepprocess Step One (rate limiting) Øconversionto acetaldehyde by alcohol dehydrogenaseØRatedetermined by availability of enzymeStep TwoØConversionof acetaldehyde to acetyl coenzyme A by aldehyde dehydrogenase (and others)Ultimately…ØAcetyl coenzyme A isbroken down into H2O and CO2 -releases energy forbodyØRemainingenzyme is used in bodily processes |
|
|
What are the two steps of alcohol elim |
Step One (rate limiting) Øconversion to acetaldehyde by alcohol dehydrogenase ØRate determined by availability of enzyme Step Two ØConversion of acetaldehyde to acetyl coenzyme A by aldehyde dehydrogenase (and others) |
|
Explain this in relation to elimination |
Step One (rate limiting) Øconversion to acetaldehyde by alcohol dehydrogenase ØRate determined by availability of enzyme Step Two ØConversion of acetaldehyde to acetyl coenzyme A by aldehyde dehydrogenase (and others) Ultimately… ØAcetyl coenzyme A is broken down into H2O and CO2 -releases energy for body ØRemaining enzyme is used in bodily processes |
|
|
Factors Affecting Elimination |
•Variablility between people(normal range is 10-20 mg/100ml of blood per hour•Rateof metabolism influenced by drinking experience•Eatingspeeds the rate of metabolism•Microsomalethanol-oxidizing system (MEOS) |
|
|
•Microsomalethanol-oxidizing system (MEOS) |
ØHandles 5-10% of metabolism ØActivity increases with consumption – may account for half of increased metabolism in heavy drinking (tolerance) ØAlso metabolizes barbiturates (heavy drinkers have resistance to these) |
|
|
Basic Neuropharmacology of alcohol |
•Higherconcentrations (1,000 to 1,000,000 times that of other drugs) required foreffect•Actsby neural transmission like other drugs•Actson many systems (pharmacology is complex)Main effects at GABAand GLU receptors but also affects systems for Glycine, 5-HT, Ach, DA, and endogenouseopioids |
|
|
GABA, •Tworeceptor types: |
GABAA & GABAB – alcohol acts at both but more known about A type |
|
|
•GABAA |
Ø8 main types of receptor subunit (among these there are 19 possible varieties of subunit) ØEach receptor complex is made up of 5 of the 19 subunits, organized in different ways à many types of GABAA receptor complex ØBrain area specific à may be important for function ØMost common type à two alpha, two beta, one gamma |
|
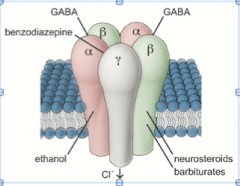
A Common GABAA receptor |
Showswhere drugs and NTs bindGABAbinds to the orthosteric (NT) sites (complexopens and CL- rushes in – inhibitscell)Alcoholbinds to allosteric sites (altersshape of receptor –increases the efficacyGABAto open the channel – does not cause channel to open;merely changes the receptorAlcoholis a positiveallosteric modulator(and a GABA agonist) |
|
|
GABA binds to the __________ (NT) sites (complex opens and ____ rushes in, ______ cell) Alcohol binds to _______ sites (alters ______ of receptor – increases the ________ GABA to open the channel – does not cause channel to _____; merely changes the receptor Alcohol is a positive allosteric _______ (and a GABA ______) |
orthosteric; CL-; inhibits; allosteric; shape; efficacy; open; modulator; agonist |
|
|
True or false GABA causes channel to open |
False, changes |
|
|
Characteristics of GABAA action |
•Alcoholacts only at receptors with a particular alpha & delta subunit combination•Thesereceptors sensitive to low levels of GABA and alcohol•Twolocations ØInpost-synaptic membrane but NOT at a GABA synapse (activated by spillover ofGABA from the synapse)à enhance long-terminhibitionØOnpresynaptic membrane where they enhance GABA release•Noticeablein the cerebellum where alcohol interferes with function of Purkinje cells à motor & balance impairment |
|
|
•Noticeablein the cerebellum where alcohol interferes with function of ______ cells ---> __________ & _________ impairment |
Purkinje; motor & balance |
|
|
•Two locations GABA a Receptors |
ØIn post-synaptic membrane but NOT at a GABA synapse (activated by spillover of GABA from the synapse)à enhance long-term inhibition ØOn presynaptic membrane where they enhance GABA release |
|
|
The GABAB Receptor |
•Metabotropic•Secondmessenger and indirect control of a K+ channel•ThreetypesØPresynapticautoreceptorØPostsynapticblocker (alters calcium channels)ØMaychange levels of cAMP (alters neuralplasticity)Ø•Alcoholaffects function at synapses where DA is released |
|
|
Glutamate Effects |
•Alcoholblocks GLU transmission••Depressesthe ion channel controlled by glutamate at the NMDA receptor••Notall NMDA receptors are subject to this depression – only those with specificcombinations of subunits (somewhat like GABA) |
|
|
Glutamate (GLU) |
•Axonterminals all over the brain•Atleast 8 GLU receptor types•Threeof these are ionotropic (kainate, AMPA,NMDA)& produce EPSPs when stimulated•Drugscan bind to the NMDA receptor (e.g.,ketamine & PCP) |
|

Glutamate NMDA receptor, how open? |
requires2 conditions:ØMembrane depol (due to nearby AMPAreceptors), tolet Mg++plug float away. GLU and glycine mustbind to open channel |
|
|
NMDA |
“double-gated” Normally blocked by Mg++ ion |
|
|
WHat happens when NMDA receptor opens? |
Whenopen, Na+ rushes inWithintense stim Ca++ (depol cell) also enters cellCa++ activates enzymes that change AMPA receptors to letmore Na+ into cell à bigger EPSP AlsoCA++ acts as a second messenger. |
|
|
WHat is NMDA recepter imp for? |
learning& memory |
|
|
Drugs can modifythis system |
Overstimulation of receptors leads to excitotoxicity |
|

How does alcohol work? |
Thereis a binding site inside the channelWhenalcohol attaches, it blocks the channel |
|
|
One effectof long term exposure: |
-brain upregulates NMDA receptor functioning (makes receptors more sensitive to GLU) -this may be responsible for later withdrawal symptoms |
|
|
thereis a balance between GABA and GLU in the CNS and alcohol disrupts it: |
•GABAstimulation depresses neural activity•GLUeffect decreases excitability••Together, they depress neural activity |
|
|
Alcohol effects on Hippocampus |
probable memory effects ØNMDA receptors contribute to long-term potentiation (for memory formation) --> Alcohol interferes ØNeurogenesis --> Alcohol prevents this |
|
|
Prefrontal Cortex |
probable cognitive effects –attention, planning, problem solving) ØEffects of alcohol mimic brain damage (impulsivity) ØGLU pyramidal projections to the rest of the brain ØGABA interneurons suppress the GLU neurons |
|
|
Mesolimbic DA system in a view of the brain |
1.In the VTA:GABAergicinterneurons normally Inhibitthe DA neurons 2.In the NA: GABAergicneurons project back to the VTAGABAergic neurons |
|
|
Alcoholenhancesthese effects byfacilitating GABA so… |
•The NA neurons release more GABA •Cells in the VTA become less active (lose their ability to inhibit DA neurons) •Increased firing and DA output |
|
|
Other effects of alcohol: |
•In the NA there are also effects of GLU •In the VTA, effects of 5-HT |
|
|
Can Alcohol Effects Be Blocked? |
mostly, NO •Adrug may antagonize the effects of alcohol in one location but not in another(e.g., RO15-4513 developed in the80s) •Adrug may partially reverse a specific effect (e.g., caffeine and some drivingeffects) --> however, drinking caffeine will not alter subjectiveeffects or return behaviour to the point wheredriving is safe (i.e., it doesn’t ‘sober you up’) •However, no drug hasbeen found that will reverse all of the effects of alcohol |
|
|
EFfects of alcohol on the body |
•Dilationof capillaries, •InhibitsADH (antidiuretic hormone) |
|
|
•Dilationof capillaries |
Øflushed face in heavy drinkers ØHeat loss from body (alcohol not useful to warm you up) |
|
|
•InhibitsADH (antidiuretic hormone) |
ØIncreased urination ØLoss of water |
|
|
•Between.05 and .10 BAC |
more talkative, higher voice pitch, mild excitement |
|
|
•Between.10 and .15 BAC |
moretalkative (and cheerful), loud, boisterous, and then sleepy |
|
|
•Above.15 BAC |
nausea, vomiting, lethargy, and stupor |
|
|
•Athigh doses (>200 mg/100 ml) |
loss of understanding, memory blackout, unconsciousness |
|
|
Complex Effects on Behaviour |
•Subjective•Perceptual•Behavioural(performance)•Memory•Driving•BehaviouralControl |
|
|
Subjective Effects |
•Sometimes“biphasic” ØStimulation(and euphoria) followed by depression/anger/sedation••Butsome individuals experience only the sedating effect••Thosewho experience both effects may be more likely to abuse alcohol (they report moreliking) |
|
|
Perceptual |
•Athigher doses à has detrimentaleffect on visionØIncreasesabsolute threshold for visionØLowersvisual acuity (flicker fusion threshold lowered)ØReducesperipheral visionØ•Reducestaste/smell sensitivity•Decreasespain sensitivity |
|
|
Performance |
•At.08 BAC, slows reaction time by 10%•ComplexRT tasks show detrimental effects at low doses•Deficitsin hand-eye coordination (e.g., on pursuit rotor task)•Earlymeasure (pre-breathalzyer) was the “RombergSway Test”ØMeasureis degree of sway from the centre line•••Atlow doses, reward can overcome some effects (see Vogel-Sprott expts in previouslectures) |
|
|
At ________, slows reaction time by 10% |
.08 BAC |
|
|
.Memory and Blackouts |
•Manystudies showing lots of effectsØMaindifficulty appears to be storage and long-term memory problemsØErrorsin visual memory occur after peak BACØErrorsin verbal memory occur after 20 min•Theseeffects become relativelypermanent with chronic use |
|
|
•Blackoutsare a form of amnesia (loss of memory for events while drunk) |
ØGrayout – remember some things, can remember more with prompting (problem of retrieval) ØEn bloc blackout (more serious) – remember nothing (ever) for a block of time, unable to form a long term memory (problem of formation) |
|
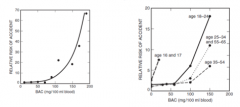
Describe |
Thesetwo graphs show overall effect of alcohol on likelihood of having an accident(overall and by age group). Notethat the trouble appears to start after .05 BAC (mostly) and definitely after.08. These types of numbers formthe basis for the .08cutoff used by many jurisdictions. |
|
|
Behavioural Disinhibition |
•Failureto stop behaviour•So,disregard for risk, social norms, and consequences of action (more concernedwith short-term gratification) - mayfacilitate tasks where anxiety interferes |
|
|
How is Behavioural Disinhibition shown Inexperiments |
by failure on the “go-stop” task (interferes with response to the stop signal |
|
|
Effects on Non-Human Animals |
•OnFI and FR schedules, alcohol increases response rate at low doses and decreasesthe rate at high doses à dose dependent••Alcoholincreases response rates after these rates have been suppressed by shock ØInother words, animals appear to show disinhibition – are less concerned aboutthe shock |
|
|
•Acutetolerance |
Øpeople appear more intoxicated during the rising phase ØHowever acute effects on cognition are variable |
|
|
•Chronictolerance |
(develops in a few weeks) Øneed 30-50% increase in dose to achieve effect |
|
|
•Metabolictolerance |
Moderate drinkers have higher tolerance than non-drinkers |
|
|
•BehaviouralTolerance |
ØShown on treadmill task in rats ØIn humans, worse cognitive performance with unfamiliar beverage compared to familiar beverage ØAction at CA++ and K+ channels may be responsible – mechanism unknown • |
|
|
“Alcoholism” |
•Termnot used in DSM – it is specific to one drug •Soit would be more appropriate to use “addicted to alcohol” •Orpreviously, ”substance abuse of alcohol” etc. •Wecommonly use the term “alcoholic” to describe the personØProdomal (early) phase is“problem drinking” à blackouts ØSomeprogress and become “gamma alcoholics” (Jellinek)à loss of control andphysical dependence |
|
|
ØProdomal (early) phase |
is “problem drinking” --> blackouts |
|
|
“gamma alcoholics” |
(Jellinek)--> loss of control and physical dependence |
|
|
•Alcoholpoisoning from a single large dose can be lethal |
ØAt .50 mg/100 ml death occurs within 2 hours ØHighest recorded BAC was 3 times this amount and achieved by drinking a large amount in a 3 hour period (this person was saved) |
|
|
•Lethaldose close to social dose |
(7.5 oz is a common social dose and 25 oz is lethal for most) --> one problem here is behavioural disinhibition |
|
|
•Causeof death is by: |
respiratory failure |
|
|
•Hangover |
not dangerous for most, but serious for those with epilepsy, heart disease, or diabetes |
|
|
•Socialharm – |
accidents, crime, damage to families & social relationships |
|
|
•Reproduction |
ØIncreased interest at low doses, reduced arousal at high doses ØIn males, low doses prolong erections ØIn males, alcohol decreases sensitivity to female social cues (friendliness vs. sexual interest) |
|
|
Harmful Effects - Chronic |
Liver; Cancer; Nervous System; Reproduction ; •Fetal Alcohol Syndrome (FAS) |
|
|
•Liver |
Øalcohol causes scarring (cirrhosis) (at 5 drinks per day for 5 yrs) |
|
|
•Cancer |
ØMouth, throat, colon, liver (perhaps due to acetylhyde) ØDissolves tobacco carcinogens ØFactor in breast cancer (for those predisposed) |
|
|
•NervousSystem |
ØKorsakoff’s Syndrome – vitamin B1 (thiamine) deficiency; results in confusion/babbling and is irreversible ØEpilepsy ØAlcohol dementia – progressive cognitive decline ØIn young people, binge drinking appears to cause memory deficits |
|
|
•Reproduction |
ØIn males --> impotence, shrinking of testicles, loss of interest ØIn females --> less documented |
|
|
•FetalAlcohol Syndrome (FAS) |
ØMechanism unknown ØCauses a series of issues – mental retardation, poor coordination, low birth weight, low muscle tone, some facial abnormalities ØIn USA, 10/1,000 live births |
|
|
Beneficial Effects |
•Hormesis – some good effectsat low doses•Riskof some diseases (e.g., heart attack, diabetes) drops at low doses but thenincreases at higher doses•Sameeffect is shown for ischemic stroke in the elderly (2 drinks per day)••”nowherein medicine is the double-edged sword so sharp on both sides” (Sandridge et al., 2004) |