Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
82 Cards in this Set
- Front
- Back
|
Horizontal axis (time)
1 small box = ____ seconds 5 small boxes = _____seconds Scores on top of graph = _____ seconds Paper speed = _____mm/sec |
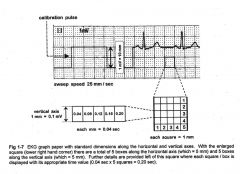
1. 0.04 seconds
2. 0.20 seconds 3. 3 seconds 4. 25 mm/sec |
|
|
Verticle axis (aplitude)
1 small box = ____mm = _____mV 10 small boxes = ___ large boxes = ______mV |
1. 1 mm = 0.1mV
2. 2 large boxes = 1.0mV |
|
|
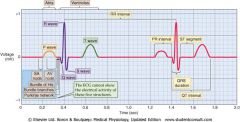
P wave (atrial depolarization)
Upright (positive) in which leads? |
I, II, AVF, and V4-6
|
|
|
P wave is normally negative in which lead?
|
AVR
|
|
|
QRS represents?
|
ventriular depolarization
|
|
|
The first downward, or negative, wave before an R wave is a _____ wave
|
Q wave
|
|
|
Any upward, or positive, was is an _______ wave
|
R wave
|
|
|
A downward, or negative, wave after an R was is an _____ wave
|
S wave
|
|
|
A "QS" wave in V1 or V2 couple represent a?
|
MI
|
|
|
The amplitude of each wave in the QRS complex is indicated by ______case letters when it is _<______ the amplitude of the entire complex
|
lower case when it is <1/3 the amplitude (qRS)
|
|
|
If the amplitude of the QRS complex is >_____ it is indicated by a ______case letter?
|
>1/3 the amplitude, upper case letter (qRS)
|
|
|
As the QRS complex progresses from V1-6, you should see what with the S wave?
|
Decreased amplitude
|
|
|
As the QRS complex progresses from V1-6, you should see what with the R wave?
|
Increased amplitude
|
|
|
List some conditions associated with poor R wave progression
|
LVH, RVH
Ant. MI Emphysema (L) BBB misplaced precordial leads |
|
|
Normal transition (R-S=same height) of the R-S complex usually occurs?
|
V3-V4
early - V1-V2 late - V5-V6 |
|
|
What is the normal QRS duration?
|
0.05-0.10 seconds
|
|
|
A prolonged QRS interval usually indicates?
|
intraventricular conduction delay
|
|
|
What might the appearance of the QRS look like with intraventicular conduction delays?
|
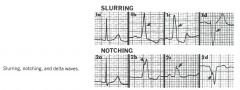
Causes the QRS to widen Slurring following the peak of the QRS
Notch at the peak of the QRS |
|

Name the type of wave and what it could represent
|
Delta wave, these occur in several pre-excitation syndromes and produce a characteristic deformity (hump or slurring) at the beginning of the QRS (ex. WPW)
|
|
|
What are 3 classic signs of WPW?
|
Short PR
Wide QRS Delta wave |
|
|
Low amplitude of the QRS complex is <_____mm in all leads
|
<10mm in all leads (<1.0mV)
|
|
|
What are medical conditions associated with low amplitude of the QRS?
|
emphysema
pericardial effusion CHF MI Amyloidosis Hypothyroidism Extreme obesity |
|
|
High amplitude of QRS complex is indicative of?
|
Hypertrophy
|
|
|
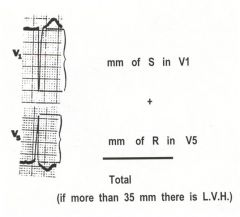
What is the calculation to measure LVH?
|
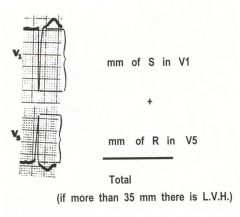
Amplitude (mm) of S in V1 + mm of R in V5 is >35 mm= LVH
(also ST depression and T wave inversion in V5 and V6) |
|
|
What are some conditions that cause LVH?
|
HTN
Aortic stenosis or insufficiency Obesity |
|
|
What would indicate RVH on the 12 lead?
|
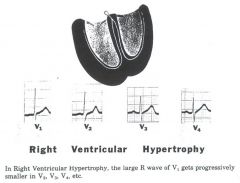
Tall R wave in V1 with progressive decrase in amplitude thru V4
|
|
|
What conditions would cause RVH?
|
COPD
Pulmonary stenosis Tricuspid insufficiency Posterior MI |
|
|
Matching
1. RVH 2. LVH a. complex looks the same, just bigger b. Complex not normal, Big R wave, small S wave |
1. B
2. A |
|
|
What constitutes a significant Q wave? What could that mean?
|
duration is >0.04 se3c and/or >1/3 the height of the QRS complex
Indicative of old MI |
|
|
In which leads do you look at the inferior part of the heart?
|
Leads II, III, aVF
|
|
|
What does the T wave represent?
|
repolarization of the ventricles
|
|
|
T waves are normally upright in which leads?
|
I, II, V3-6
|
|
|
T wave is normally inverted in which lead(s)?
|
aVR
|
|
|
What are tall T waves associated with?
|
K+ excess (tented T_
myocardial ischemia ventricular overload antypsychotic drugs CVA's or CNS ischemia |
|
|
Primary T wave inversion is frequently caused by?
|
myocardial ischemia and inflammation
|
|
|
Secondary T wave abnormalities can be caused by?
|
conduction disturbances, and LVH. Don't misdiagnose as ischemia, look at amplitude of QRS to diagnose LVH (>35mm)
|
|
|
U waves are best seen in which leads?
|
V3-4, more prominent in bradycardia and hypokalemia
|
|
|
What is a U wave?
|
a low voltage deflection of uncertain origin
|
|
|
How do you measure the PR interval?
What is normal PR interval? |
- beginning of the P to beginning of the QRS
-0.12 - 0.20 sec |
|
|
What does the PR interval measure?
|
AV node conduction
|
|
|
How do you measure the ST segment?
|
From the end of the QRS to the start of the T wave
|
|
|
An elevation of the ST segment of <____mm or a depression of <0.5mm may be considered normal
|
1. <1mm
2. <0.5mm |
|
|
What is the J point? Why is it important?
|
The junction of the S wave and the ST segment
Important in determining myocardial ischemia |
|
|
To evaluate ST segment elevation or depression you will measure where in relation to the J point?
|
0.06mm or 1 1/2 blocks after J point.
|
|
|
Elevation of the ST segment at the J point may be a normal variant in which types of patients?
|
children, young adults and black men due to early repolarization
|
|
|
Where do you measure the QT interval from? What does it represent?
|
The beginning of the Q to the end of the T
Total time of systole |
|
|
The QT interval shouild not be < or > half the preceding R-R interval if the HR is between 60-90?
|
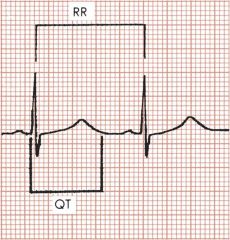
>half - may predispose the the patient to R and T (Torsades de Points)
|
|
|
The QT duration is normally correct for the HR to = QTc. What is the normal QTc?
|
0.44 +/- 0.02 seconds
|
|
|
What is the normal ECG deflection?
|
Down and to the left
|
|
|
Vectors are used to represent the hearts?
|
Hearts electrical activity
Has a force that has both magnitude and direction |
|
|
Vectors are caused by?
|
The spread of the wave of depolarization throughout the myocardium
|
|
|
What is a lead?
|
an electrode used to sense the hearts electrical activity
|
|
|
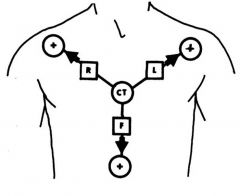
What are the 3 basic laws of electrocardiography?
|
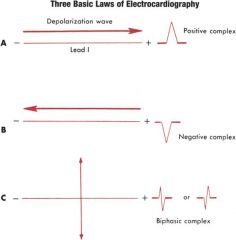
-Positive - when depolarization is directed toward the + electrode
-Negative - when depolarization is directed away from the + electrode -Biphasic deflection - when depolarization is directed perpendicular to the + electrode. |
|
|
What are the frontal plane hexaxial leads of the 12 lead?
|
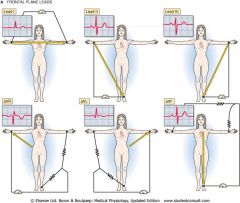
Bipolar Limb Leads I, II, III
Augmented Limb Leads aVR, aVL, aVF |
|
|
The Bipolar limb leads form?
|
Einthovens triangle with the heart located in the center
|
|
|
Einthovens Law is the sum of?
|
Any complex in leads I and III equals that of Lead II (this is why P waves are best viewed in Lead II)
|
|
|
What does the aVR look at?
|
Nothing all - complexes
|
|
|
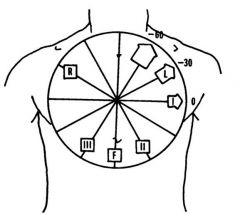
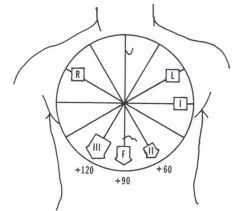
The frontal plane is divided into ______segments each _____degrees each?
|
12 segments, 30 degrees each
|
|
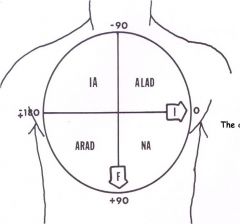
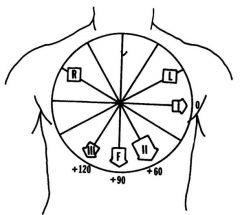
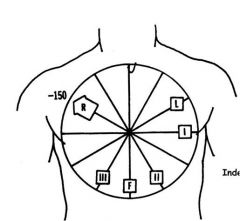
In the Hexaxial lead system, label the frontal leads
|
|
|
|
Augmented leads are unipolar with the + pole at? - pole?
|
Einthoven's triangle
- pole is the theoretical electrically neutral center of the heart |
|
|
What are the augmented limb leads?
|
aVR
aVL aVF |
|
|
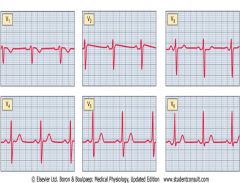
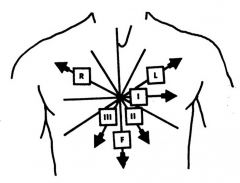
What are the 6 horizontal plane precordial leads and which part of the heart to they look at?
|
V1 - septum, or R heart
V2 - septum, or R heart V3- anterior wall V4 - anterior wall V5 - lateral wall V6 - lateral wall |
|
|
What are the lead locations for the precordial leads?
|
V1 - 4th ICS, RSB
V2 - 4th ICS, LSB V3 - midway between V2 and V4 V4 - 5th ICS midclavicular line V5 - 5th ICS anterior axillary line V6 - 5th ICS mid axillary line |
|
|
Why does the R wave normally enlarge as you go from V1-V6?
|
Left ventricle is biggest, thickest so you get more eletrical current
|
|
|
Which area of the heart of you looking at with the Brown lead?
|
The "Brown" lead is the "V" lead so you place it at the part of the heart you want to look at
|
|
|
Whaqt is the numerical degree designation of each of the 6 limb leads?
|
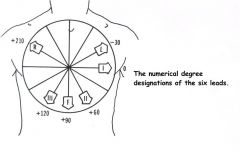
I = 0 degrees
II = +60 degrees III = +120 aVL = -30 degrees aVF = +90 aVR = -150 |
|
|
What are the locations of the
1. Normal axis 2. Right axis deviation 3. Left axis deviation 4. Indeterminate axis deviation |
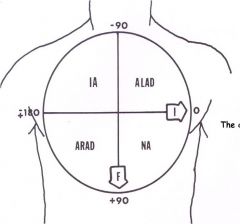
Normal axis = 0 to +90degrees
RAD = +90 to +180 degrees LAD = 0 to -90 degrees Intererminate axis = -90 to -180 (represents extreme R axis deviation) |
|
|
What is the Quick Quadrant method for determining the axis of the QRS complex?
|
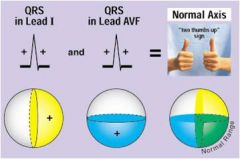
Lead I: indicates if depolarization is moving to the R or L of the heart
Lead aVF: indicates if depolarization is moving predominately upward or downward |
|
|
What is the Precise Method for determining axis deviation, what are the 3 essential questions?
|
1. which lead records the tallest most + QRS
2. Which lead records the most - QRS complex 3. Which lead records the smallest or most biphasic (RS) QRS complex? |
|
|
List some causes of right axis deviation?
|
Normal in tall, slender people, infants and children
RVH Conduction disturbances (WPW, RBBB) Myocardial infarction (anterior, anterolateral) Valvular disease (right sided) Pulmonary Htn Congenital heart disease Pulmonary conditions |
|
|
List some causes of left axis deviation?
|
Normal variant in obese, pregnant or elderly
LVH Conduction -WPW, LBBB MI - inferior Valvular disease L side Systemic HTN Congenital heart disease Abdominal tumor Ascites |
|
|
Matching:
1. limb leads 2. augmented limb leads 3. precordial leads a. unipolar b. bipolar |
1. b -bipolar
2. a - unipolar 3. a - unipolar |
|
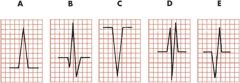
Name the complexes
|
1. R
2. qRS 3. QS 4. RSR' 5. QR |
|
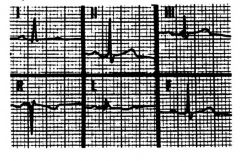
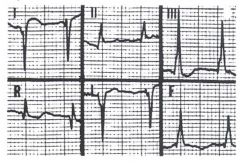
Determine axis
|
Normal axis
|
|
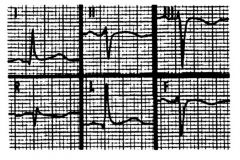
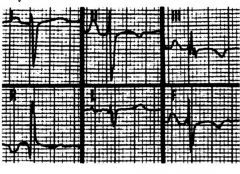
Determine axis
|
Left axis
|
|
Determine axis
|
Right axis
|
|
Determine axis
|
Indeterminate axis
|
|
|
What is the isoelectric line?
|
-The baseline of the ECG tracing
-No electrical activity occuring -associated with the PR interval -Deflections above + - Deflections below - |
|
|
What is considered high amplitude in the following leads
1. aVL 2. aVF 3. V1-6 |
1. >11 mm in aVL
2. >20 mm in aVF 3. > 30 mm in V1-6 |
|
|
In progression from V1-V6 describe the normal progression of amplitude in the following waves
1. R 2. S 3. T |
1. Bigger
2. Smaller 3. Bigger |
|
|
What waves does the 3 basic laws of ECG apply to?
|
P wave (artial depolarization)
QRS complex (ventricular depolarization) (p 13 of handout) |
|
|
The intersection of what leads divide the precordium into 4 quadrants?
|
Leads I and aVF
|