![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
107 Cards in this Set
- Front
- Back
|
What does static posture represent? |
The alignment of the body's segments, or how the person holds him or herself "statically" or "isometrically" |
|
|
What type of muscles help with proper postural position? |
The deeper muscles that contain greater concentrations of type I (slow twitch) muscle fibers and function to hold static positions of low-grade isometric contractions for an extended period of time. |
|
|
What is good posture defined as? |
the state of musculoskeletal alignment and balance that allows muscles, joints, and nerves to function efficiently. |
|
|
What insights does a static posture assessment provide? |
Muscle imbalance at a joint and the working relationships of muscles around a joint (muscle imbalance often contributes to dysfunctional movement)
Altered neural action of the muscle moving and controlling the joint (for example, tight or shortened muscles are often overactive and dominate movement at the joint, potentially disrupting healthy joint mechanics.)
|
|
|
What is Kyphosis? |
Increased posterior thoracic curve from neutral (Hunchback) |
|
|
What is lordosis? |
Increased anterior lumbar curve from neutral - Lower back curves toward the front
|
|
|
What is scoliosis? |
Lateral spinal curvature often accompanied by vertebral rotation. |
|
|
What is flat back? |
Decreased anterior lumbar curve |
|
|
What is sway back? |
Decreased anterior lumbar curve and increased posterior thoracic curve from neutral |
|
|
What are muscle imbalances associated with Kyphosis-lordosis posture? |
Facilitated/Hypertonic (shortened) are tighter: Hip flexors Lumbar extensors Front chest/shoulders Latissimus dorsi Neck extensors Inhibited (lengthened): Hip extensors External obliques Upper-back extensors Scapular stabilizers Neck flexors |
|
|
What are the NON-correctable factors for muscle imbalance and postural deviations? |
Congenital conditions (e.g. scoliosis) Some pathologies (rheumatoid arthritis) Structural deviations (tibial of femoral torsion or femoral ante version) Certain types of trauma (surgery, injury) |
|
|
What does proper postural alignment promote? |
Optimal neural activity of the muscles controlling and the moving the joints.
the length-tension relationships and force-coupling relationships function efficiently. Allows body to generate acceptable forces throughout the kinetic chain |
|
|
What is the right-angle rule? |
Looking at static posture. A state in the frontal plane where two hemispheres are equally divided and in the sagittal plane wherein the anterior and posterior surfaces appears in balance (taking a person, placing a string overhead, have them face forward with the line cutting them right down the middle between the breasts,etc. then having them turn around with the line going down the middle and then to their side with the line going down the middle |
|
|
What information should be collected for the postural alignment? |
Health history and lifestyle info -> static postural analysis -> identify correctible postural compensations/adminstration appropriate screen movements -> phase 1 stability and mobility |
|
|
What is the first deviation that should be looked at during postural assessments? |
Ankle pronation/supination and the effect of the tibal and femoral rotation. |
|
|
What is pronation and supination? |
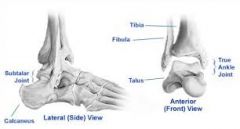
Pronation is arch flattening. Supination is high arches at the subtalar joint |
|
|
Because the body is one continuous kinetic chain, the position of the subtalar joint will impact the position of tibia and femur. What does a pronated subtalar joint force?
|
Internal rotation of the tibia and slightly less internal rotation of the femur. This also force rotation of the knee and places additional stresses on some knee ligaments and the integrity of the joint itself. As pronation tends to move the calcaneus (heel) into eversion, this may lift the outside of the heel slightly off the ground (plantar flexion)
|
|
|
What does planter flexion cause? |
Tightening of the calf muscles and potentially limit ankle dorsiflexion |
|
|
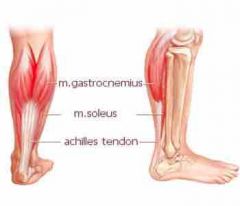
Pronation causes tight calf muscles. What does a tight gastrocnemius (calf muscle) and soleus complex (lower calf) do? |
Force calcaneal (heel) eversion and in an otherwise neutral subtalar joint position. |
|
|
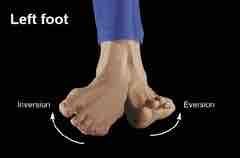
What are the effects of pronation of the foot, tibial (knee) femoral movements? |
Internal rotation |
|
|
What are the effects of supination of the foot, tibial (knee) femur movements? |
External rotation |
|
|
What is the second deviation that will be assessed during postural observations? |
Hip adduction |
|
|
What are the effects of pronation of the foot, tibial (knee) femoral movements? What is the plane of view? |
Foot movement- Eversion Tibial (knee) and femur -Internal rotation Plane of view - View from the front |
|
|
What are the effects of supination of the foot, tibial (knee) femoral movements? What is the plane of view? |
Foot movement- Inversion Tibial (knee) femur movement- External rotation Plane of view- View from the front |
|
|
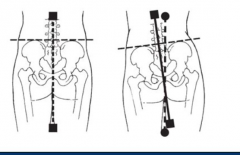
When does anterior tilting of the pelvis occur? |
Individuals with tight hip flexors, which is generally associate with sedentary lifestyles. With standing this pulls the pelvis into a front tilt (top and front portion of the pelvis rotates downward) |
|
|
What will anterior/front tilting do to the spine? |
Increase lordosis |
|
|
What is the Rotation, muscles that are tight, suspected lengthened muscles and plane of view for an anterior pelvic tilt? |
Rotation- ASIS tilts downward and forward Muscles suspected to be tight- Hip flexors and erector spinae (runs along middle of back) Muscles suspect to be lengthened- Hanstrng, rectus abdomens Plane of view- Sagittal |
|
|
What is the Rotation, muscles that are tight, suspected lengthened muscles and plane of view for an posterior pelvic tilt (cross syndrome)? |
Rotation- ASIS tilts upward and backward Muscles suspected to be tight- Rectus abdomens Muscles suspected to be lengthened- hip flexors Plane of view sagittal |
|
|
What is the fourth deviation when observing posture? |
Shoulder position and thoracic spine |
|
|
What is scapular protraction? |
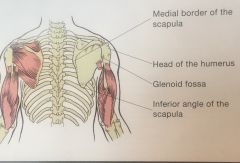
Protrusion of the vertebral (medial) border outward |
|
|
What is scapular winging? |
Protrusion of the the inferior angle and vertebral (medial) border outward |
|
|
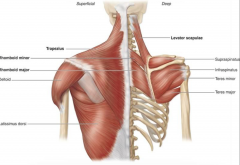
What muscles are suspected to be tight if the shoulders are aren't level? |
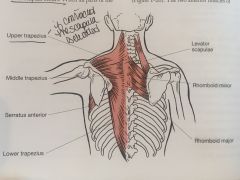
Upper traps, levator scapula, rhomboids
View- Frontal |
|
|
What muscles are suspected to be tight if their is asymmetry to midline? |
Lateral trunk flexors (flexed side)
View- frontal |
|
|
What muscles are suspected to be tight if the shoulders are protracted/abduction (rounded up shoulders)? |
Serratus anterior, anterior scapulohumeral muscles, upper trap View- Sagittal |
|
|
What muscles are suspected to be tight if the shoulder position is medially rotated humerus (upper arm bone) rotated in? |
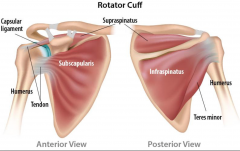
Pectorals major and latissimus dorsi (shoulder adductors), subscapularis
View- Frontal |
|
|
What muscles are suspected to be tight if the shoulder position is kyphosis and depressed chest? |
Shoulder adductors, pectorals minor, rectus abdomens, internal oblique View - Saggital |
|
|
What is the fifth deviation assessed? |
Head position |
|
|
What is considered good head postural head position? |
Earlobes are aligned approx over the acromion process |
|
|
What is a common altered head position? |
Forward head position, does not tilt head downward but shifts it forward so that the earlobe appears significantly forward of the acromioclaviccular (AC) joint |
|
|
What view should be used in viewing head position? |
Saggittal |
|
|
What muscles are suspected to be tight if their is observed forward head position? |
Cervical spine extensors, upper trap, levator scapulae |
|
|
Why is observing movement important? |
It is an effective method to determine the contribution the muscle imbalance and poor posture have on neural control and helps identify movement compensations |
|
|
What are the five movements that people perform during many daily activities? |
Bending/raising and lifting/lowering Single-leg movements Pushing movements Pulling movements Rotational movements |
|
|
What is the objective, equipment and instructions for a bend and lift screen? |
objective- to examine symmetrical lower-extremity mobility and stability, and upper extremity stability during a bend-and-lift movement
Equipment- 2 to 4 for dowels or broomsticks
Instructions- Ask the client to perform a series of basic bend-and-lift movements (squatting movements) |
|
|
Feet -In the B & L screening view , issues, key overactive tight muscle and underactive (lengthened) muscles |
View- Anterior Issue-lack of foot stability: Ankles collapse in feet turn out Tight muscles- Soleus, lateral gastrocnemius, peroneals Lengthened muscles- Medial gastrocnemius, gracilis, sartorial, tibias group
|
|
|
Knees- B & L screening what is the view , issues, key overactive tight muscle and underactive (lengthened) muscles for a joint location of knees |
Anterior Knees move inward Then Hip adductors, tensor fascia latte are tight Lengthened- Gluteus medias and maximus |
|
|
Torso in the B & L screening what is the view , issues, key overactive tight muscle and underactive (lengthened) muscles |
Anterior Lateral shift to a side Tight- Side dominance and muscle imbalance due to potential lack of stability in the lower extremity during joint loading |
|
|
SIDE foot view In the B & L screening what is the view , compensation, key overactive tight muscle and underactive (lengthened) |
Unable to keep heels in contact with the floor Tight- Plantarflexors Lengthened - None |
|
|
Side view hip and knee B & L screening what is the compensation, key overactive tight muscle and underactive (lengthened) |
Compensation-Initiation of movement Tight- Movement initiated at knees may indicate quads and hip flexors dominance, as well as insufficient activation of the gluteus group |
|
|
In the B & L screening what is the view , compensation, key overactive tight muscle and underactive (lengthened) muscles for a joint location of tibia and torso relationship Contact behind the knee |
View- Sagittal Compensation- Unable to achieve parallel between tibia and torso Hamstrings contact back of calves Tight muscles- Poor mechanics, lack of dorsiflexion due to tight planter flexors (which normally allow the tibia to move forward) |
|
|
In the B & L screening what is the view , compensation, key overactive tight muscle and underactive (lengthened) muscles for a joint location of lumbar and thoracic spine |
View - Sagittal Compensation: Back excessively arches Back rounds forward
Tight- Hip flexors, back extensors, latissimus dorsi
Lastissimu dorsi, trees major, pectorals major and minor
Lengthened (underactive)-- Core, rectus abdominus, gluteal group, hamstrings.
Upper back extensors. |
|
|
In the B & L screening what is the view , compensation, key overactive tight muscle and underactive (lengthened) muscles for a joint location of head |
View- Saggital Compensation- downward Upward Tight- Increased hip and trunk flexion Compression and tightness in cervical extensor region |
|
|
What does lumbar dominance in a squat movement mean?
|
This implies lack of core abdominal and gluteal muscle strength to counteract the force of the hip flexors and erector spinae as they pull the pelvis forward and during the squat movement. In this scenario, the individual experiences excessive loads within the lumbar spine as it moves into extension during the squat. The muscles of the abdominal wall and gluteal complex do not contribute enough in this situation to spare the back and foster proper execution of the squat. Chronically high hip flexors, such as those experience by those who sit all day, may contribute to this problem |
|
|
What does quad dominance in a squat movement mean? |
This implies reliance on loading the quads groups during a squat forward, creating shearing forces across the knee as the femur slides over the tibia. In this lowered position, the glute max does not eccentrically load and cannot generate much force during the upward phase. Places greater loads on the ACL. |
|
|
What does glute dominance in a s squat movement mean? |
This implies reliance on eccentrically loading the gluteus maximus during a squat movement. The first 10 to 15 degrees of the downward phase are intimated by pushing the hips backward, creating hip-hinge, the lowered position, this maximized the eccentric loading the gluteus maximus to generate significant force during the upward, concentric phase. This is the preferred method of squatting, as it spares the lumbar spine and relieves under stress on the knees. Glute dominance also helps activate the hamstrings, which pull the posterior surface of the tibia and help unload the ACL to protect if from potential injury |
|
|
What is the objective, equipment/instructions and interpretations for a hurdle step screen? |
Objective- To examine simultaneous mobility of one limb and stability of the contralateral limb while maintaining both hip and torso stabilization during a balance challenge of standing on one leg. Equipment/Instructions; String to step-over and a plastic rod. Instruct client to load onto one leg and slowly lift the opposite leg over the string, flexing the hip to clear the strong before returning to starting. Do the other leg. |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step looking at the feet? |
Compensation- Lack of foot stability; supination or pronation Tight- Soleus, lateral gastrocnemius, peroneals Underactive- Medial gastrocnemius, gracilis, sartorius, tibias group, gluteus medium and maximus- inability to control internal rotation |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step looking at the knees |
Compensation - Move inward Tight- Hip adductors, tensor fascia latea Underactive- Gluteus medius and maximus |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step looking at the hips |
Compensation- Hip adduction > 2 inches Stance- leg hip rotation Tight- Hip adductors, tensor fascia latae Stance- Leg or raised-leg internal rotators Underactive- Gluteus medius and maximus Stance- leg or raised-leg external rotators |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step with a joint location at the torso
|
Compensation- Lateral tilt, forward lean, rotation
Tight- Lack of core stability |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step with a joint location at the raised-leg |
Compensation- Lack of ankle dorsiflexion Limb deviates from sagittal plane Hiking the raised hip Tight- Ankle plantar flexors Raised leg- hip extensors Stance-leg hip flexors-limiting posterior hip rotation during raise Underactive- Ankle dorsiflexors raised hip flexors |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the hurdle step with a joint location at the pelvis and low back |
If there is a: Anterior tilt forward torso lean Posterior tilt with hunted over torso
Tight- Stance-leg - hip flexors Rectus abdominus and hip extensors
Underactive- Rectus abdominus and hip extensors Stance leg- hip flexors
|
|
|
What is the objective, instructions and observations for a shoulder push stabilization screen? |
objective- To examine stabilization of the scapulothoracic joint and core control during closed-kinetic-chain pushing motion. Instruction- Client does a push-up to full arm extension Observation- Observe any notable changes in the position of the scapulae relative to the rib cage at both end-ranges and the lumber hyperextension in the press position |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the shoulder push with a joint location at the scapulothoracic? |
View- sagittal Compensation- Exhibits winging during the push-up Key suspected compensations- Inability of the parascapular muscles to stabilize the scapula against the rib cage. Can also be due to a flat thoracic spine |
|
|
What is the view, compensation, tight muscle and lengthen (underactive) muscle in the shoulder push at the trunk? |
Compensation- Hyperextension or "collapsing' of the low back.
Key suspected compensations- Lack of core, abdominal and low-back strength, resulting in instability |
|
|
What is the objective, equipment/instructions, and interpretations of the thoracic spine mobility screen? |
Objective- To examine bilateral mobility of the thoracic spine. Lumbar spine rotation is considered insignificant, as it only offers approx 15 degrees of rotation. Instructions/equipment- Sit on chair, block between knees, hold poll in crossed arms at shoulders. Rotate left and right |
|
|
What are the view, compensation and possible biomechanics problems at the trunk joint for a thoracic spine mobility screen? |
View- Transverse Compensations- None if trunk rotation achieves 45 degrees in each direction |
|
|
What are the view, compensation and possible biomechanics problems at a trunk joint location for a thoracic spine mobility screen? |
View- Transverse Compensations- Bilateral discrepancy (assuming no existing congenital issues in the spine) Possible Problems- Side- dominance, differences in paraspinal development, torso rotation, perhaps associated with some hip rotation Note; Lack of thoracic mobility will negatively impact glenohumeral mobility. |
|
|
What is the Thomas test, the objective, equipment/Instructions? |
Tests hip flexion and quad length
Objective- to assess the length of the muscles involved in hip flexion. This test can actually assess the length of the primary hip flexors (not for client's with low back pain) Instructions- Have client lay on table with edge of tables at knees, Grab under the knee and pull at a 90 degree angle |
|
|
What is the suspected muscle tightness with the back and sacrum flat, the back of the lowered thigh does not touch the table and the knee does not flex to 80 degrees |
Primary hip flexor muscles |
|
|
What is the suspected muscle tightness with the back and sacrum flat, the back of the lowered thigh does not touch the table, but the knee does flex 80 degrees? |
The iliopsoas, which is preventing the hip from rotating posteriorly and inhibiting the thigh from being able to touch the table |
|
|
What is the suspected muscle tightness with the back and sacrum flat, the back of the lowered thigh does touch the table, but the knee does not flex to 80 degrees? |
The rectus femurs, which does not allow the knee to bend. |
|
|
What is the objective and instructions for a passive straight-leg raise? |
Objective- To assess the length of the hamstrings Instructions- Client lay on table. Place one hand under client's calf of the leg that will be raised and slide the other hand under the lumbar spine. |
|
|
What is the hamstring length during a passive straight-leg stretch if the raised leg achieves greater than 80 degree of mvmt before pelvis rotates posteriorly? |
Normal hamstring length
|
|
|
What is the hamstring length during a passive straight-leg stretch if the raised leg achieves less than 80 degrees of movement before the pelvis rotates posteriorly or there are any visible signs in the opposite leg lifting off the mat or table. |
Tight hamstring |
|
|
What is the objective and instructions for a shoulder flexion and extension test? |
Objective- To assess the degree of shoulder flexion and extension. This should be performed in conjunction with the Apley's scratch test.
Instructions flexion- lay on a mat, knees bent, arms at the sides. Raise both arms into shoulder flexion, moving them overhead
Shoulder extension lie prone (on their stomach) and slowly raise both arms into extension |
|
|
What is the shoulder mobility if the flexion of the shoulders is 170-180 degrees (hands touching/nearly touching the floor)? |
Good shoulder mobility |
|
|
What is the shoulder mobility if the flexion of the shoulders is to 170 or there are discrepancies between the limbs |
Potential tightness in the pectorals major and minor, latissimus dorsi, tres major, rhomboids, and subscapularis. Tightness in the latissimus dorsi will force lower back to arch Tightness of the pectoralis minor may tilt the scapulae forward (anterior tilt) and prevent the arms from touching the floor. Tight abdominals may depress the rib cage, tilting the scapulae forward (anterior tilt) and prevent the arms from touching the floor. Thoracic kyphosis may round the thoracic spine and prevent the arms from touching the floor. |
|
|
What is the shoulder mobility if the extension is to 50-60 degrees off the floor? |
Good shoulder mobility |
|
|
What is the shoulder mobility if the extension is to 50 degrees or there are discrepancies? |
Potential tightness in pectoralis major, abdominals, subscapularis, certain shoulder flexors (anterior deltoid), coracobrachialis, and biceps bronchi Tightness in abs may prevent normal extension of the thoracic spine and rib cage Tightness in the biceps brachia may prevent adequate shoulder extension with an extended elbow (but may permit extension with a bent elbow) |
|
|
Which shoulder joint is designed to offer greater stability with less mobility? |
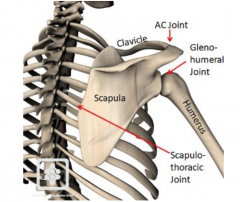
Scapulpthoracic |
|
|
Assessment of internal and external rotation of the humerus an shoulder objective? |

To assess internal (medial) and external (lateral) rotation of the humerus at the shoulder joint. Measure the degree of movement in each direction. Have client lie on their back (supine), abduct arms to 90 degrees, with 90 degree bend at elbows. Remain aligned with shoulders. Backs of the upper arm should stay against mat. |
|
|
Ability to externally rotate the forearms 90 degrees (up) to touch the mat and the inability? |
Ability= good mobility in the internal rotators. Inability= Potential tightness in the internal rotates (subscapularis) or the joint capsule an ligaments may also be tight and limit rotation |
|
|
Ability and inability to internally (lower) forearms 70 degrees toward the mat |
Ability= Good mobility Inability= Potential tightness in the external rotators of the arm (i.e. infraspinatus and teres minor) or joint capsule and ligaments may also be tight and limit rotation |
|
|
What does Apley's scratch test objective and instructions? |
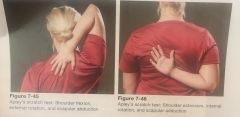
To assess simultaneous movements of the shoulder girdle (primarily scapulothoracic and glenohumeral joints)
|
|
|
What does the ability to touch specific landmarks and the inability suggest? |
Ability- Good shoulder mobility Inability- Requires further evaluation to determine the source of the limitation (i.e. which of the movements is problematic)- shoulder flexion and extension -internal ore external rotation of the humerus - scapular abduction and adduction |
|
|
What is the Sharpened Romberg test's objective and instructions? |
To assess static balance by standing with reduced base of support while removing visual sensory information. Have the client cross arms over chest, walk like a tight rope a few times then do it with eyes closed. The inability to reach 30 seconds is indicate ve of inadequate static balance |
|
|
What is the Stork stand behind test's objectives and instructions? |
To assess static balance by standing on one foot in a modified stork-stand position (yoga tree position) Poor is less than 10 seconds Excellent is greater than 30 sec in females. Males are 20 and 50 |
|
|
Why is the McGills Torso Test Battery include three tests? |
The assessment of the interrelationships among the results of the three torso test. The tests are performed individually, but then evaluated collectively |
|
|
What is the objective and instructions of the trunk flexor endurance test? |
Test muscular endurance of the deep core muscles (transverse abs, quadrates lumborum and erector spinae) It is a timed test involving a static, isometric contraction at the anterior muscles. Have the client seated on the floor and lift a step board up to a 60 degree angle. Pull the board away |
|
|
What is the objective and instructions of the trunk (side) lateral endurance test? |
Assess muscular endurance of the lateral core muscles (i.e. transverse abs, obliques, quadrates, and erector spinae. Hold a side plank |
|
|
What is the objective and instruction of the extensor endurance test? |
Used to assess muscular endurance of the torso extensor muscles (erector spinae, longissimu, iloiocostalis and multifid) Lay on a table with lower torso on and upper off and hold the upper torso flat. |
|
|
Flexion:Extension ratio should be less than? |
1.0 |
|
|
Right-side bridge:Left-side bridge should be no greater than? |
Be no greater than 0.05 from a balanced score of 1.0 |
|
|
Side bridge (either side): extension ratio should be less than? |
0.75 |
|
|
Tight muscles in Lordosis and Kyphosis? |
Hip extensors Anterior chest and shoulders Latissimus Dorsi Lumbar extensors Neck extensors |
|
|
What muscles are lengthened in Lordosis and kyphosis? |
Hip Extensor External Obliques Neck Flexors Upper Back extensor Scapular Stabilizer |
|
|
Anterior Tilting of Pelvic Bone has the pelvis tilted? |
Forward and downward |
|
|
Anterior Tilting of Pelvic Bone has the pelvis tilted? |
Forward and downward |
|
|
What muscles are tight and lengthened when there is an anterior tilting of the pelvis? |
Tight- Hip flexor Erector Spinae
Lengthened Hamstring Rectus Abdominus |
|
|
Anterior Tilting of Pelvic Bone has the pelvis tilted? |
Forward and downward |
|
|
What muscles are tight and lengthened when there is an anterior tilting of the pelvis? |
Tight- Hip flexor Erector Spinae
Lengthened Hamstring Rectus Abdominus |
|
|
What is the position of the pelvis in a posterior tilt? |
Backward and downward |
|
|
Anterior Tilting of Pelvic Bone has the pelvis tilted? |
Forward and downward |
|
|
What muscles are tight and lengthened when there is an anterior tilting of the pelvis? |
Tight- Hip flexor Erector Spinae
Lengthened Hamstring Rectus Abdominus |
|
|
What is the position of the pelvis in a posterior tilt? |
Backward and downward |
|
|
What muscles are tight and lengthened in a posterior tilting of the pelvis? |
Tight- Rectus Abdominus Hamstring Lengthened- Hip Flexor Erector Spinae
|