Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
80 Cards in this Set
- Front
- Back
|
___ vessels lack a basement membrane => lose cell to cell junction
(they aren't present in muscle, bone, tendon, or brain) |
___ vessels lack a basement membrane => lose cell to cell junction
(they aren't present in muscle, bone, tendon, or brain) |
|
|
Elderly male hypertensive smoker presents to ED c/ sx of lower extremity ischemia
-Must r/o _ |
Abdominal aortic aneurysm:
-Normal aorta 2-3 cm -Aneurysms are 2/2 medial degeneration, most commonly from ATHEROSCLEROSIS -Usually found incidentally -RFs: HTN, male, smoking, elderly -Can present c/ rupture, distal embolization -> lower extremity ischemia, compression of adjacent organs |
|
|
decrease in type _ collagen is found in familial forms of AAA
|
Proteolytic activity in the media and the collagen scaffold structure of the adventitia has been thought to contribute to AAA formation. This includes increase in matrix metalloproteinase (MMP) 9 and 1. IL-1 beta and TNF-alpha, which are secreted by inflammatory cells, are found to be elevated in aneurysm wall. Protease inhibitors (TIMP-1 and TIMP-2)are decreased. A decrease in type III collagen in aortic media has been reported in familial forms of AAA.
|
|
|
AAA repair: 3 indications
|
AAA:
-Repair if symptomatic, >5 cm, or growth >0.5cm/hr -Reimplant IMA if backpressure <40 mmHg (poor backbleeding), previous colonic surgery, stenosis @ SMA, or inadequate flow to L colon -Ligate bleeding lumbar arteries -Maintain flow to at least one internal iliac artery to avoid vasculogenic impotence |
|
|
what is the major vein injury 2/2 cross-clamping during AAA repair?
|
Complications after AAA repair:
-Retroaortic renal vein injury 2/2 proximal cross-clamp -Impotence in 1/3 due to disruption of autonomic nerves + vessels to pelvis -Graft infection rate 1% -Pseudoaneurysm after graft placement 1% -Atherosclerotic occlusion = #1 late complication after aortic graft placement -Diarrhea (esp bloody) suggests ischemic colitis -L colon ischemia 2/2 sacrifice of inferior mesenteric artery (Dx: endoscopy or ab CT; rectum spared; in no peritoneal signs => follow closely; if peritoneal signs => colectomy + colostomy) -5% mortality c/ elective repair -#1 cause of acute death after surgery = MI -#1 cause of late death after surgery = renal failure |
|
|
Most common late complication after AAA graft placement
|
Complications after AAA repair:
-Retroaortic renal vein injury 2/2 proximal cross-clamp -Impotence in 1/3 due to disruption of autonomic nerves + vessels to pelvis -Graft infection rate 1% -Pseudoaneurysm after graft placement 1% -Atherosclerotic occlusion = #1 late complication after aortic graft placement -Diarrhea (esp bloody) suggests ischemic colitis -L colon ischemia 2/2 sacrifice of inferior mesenteric artery (Dx: endoscopy or ab CT; rectum spared; in no peritoneal signs => follow closely; if peritoneal signs => colectomy + colostomy) -5% mortality c/ elective repair -#1 cause of acute death after surgery = MI -#1 cause of late death after surgery = renal failure |
|
|
What is the benefit of endovascular AAA repair?
|
Endovascular AAA repair =>
lower peri=op complication rates, but long-term outcomes unknown |
|
|
Bloody diarrhea + abdominal distension 4 days s/p AAA repair.
Suspect _ Next step _ |
Ischemic colitis after AAA repair:
-Inferior mesenteric artery ligation -> L colon ischemia -Rectum spared b/c inferior + middle rectal come off the internal iliac artery, not the inferior mesenteric -Dx: endoscopy (sigmoidoscopy - must go past rectum, into sigmoid + descending colon to splenic flexure) or abdominal CT -If clinical suspicion is equivocal (e.g. pt on pressors + risk for embolus), do angiogram to eval non-occlusive vs. occlusive mesenteric ischemia -No peritoneal signs => follow closely -Peritoneal signs => colectomy + colostomy |
|
|
AAA rupture:
<5 cm => _% in 5 yrs 5-7 cm => _% >7 cm => _% -Increased risk if 2 medical conditions... |
AAA rupture:
<5 cm => 20% in 5 yrs 5-7 cm => 33% >7 cm => 95% -Increased risk if HTN, COPD |
|
|
AAA rupture: 2 comorbidities that are the biggest predictors of rupture
|
AAA rupture:
-Leading cause of death s/ operation -Back, abdominal pain -> profound hypotension -Dx: US or ab CT -CT ab (+) for rupture: retroperitoneal fluid, extraluminal contrast -5 cm => 15-20% 5-yr risk of rupture ->8 cm => 100% risk of rupture in 5 yrs -Most likely to rupture on L posterolateral wall, 2-4 cm below renals -Major predictors of expansion, rupture: diastolic HTN, COPD -50% mortality c/ rupture IF pt reaches hospital alive |
|
|
AAA is most likely to rupture @ location _
|
AAA rupture:
-Leading cause of death s/ operation -Back, abdominal pain -> profound hypotension -Dx: US or ab CT -CT ab (+) for rupture: retroperitoneal fluid, extraluminal contrast -5 cm => 15-20% 5-yr risk of rupture ->8 cm => 100% risk of rupture in 5 yrs -Most likely to rupture on L posterolateral wall, 2-4 cm below renals -Major predictors of expansion, rupture: diastolic HTN, COPD -50% mortality c/ rupture IF pt reaches hospital alive |
|
|
ACAS study demonstrated that CEA reduces stroke rate from 11% to 5% if >__% stenosis
|
Asymptomatic Carotid Atherosclerosis Study (ACAS) 1995: asymptomatic carotid stenosis of 60% or greater by CA.
-Medical tx => 11% 5-yr risk of ipsilateral stroke, 5% for medical+ surgery group |
|
|
_ = #1 site of of peripheral obstruction 2/2 acute arterial embolism
|
Acute arterial embolism:
-Usually no collaterals, signs of chronic limb ischemia, hx claudication (unlike with thrombosis) -Sx: pain, pallor, pulselessness, paresthesia, poikilothermia, paralysis #1cause = a fib (others: LV aneurysm c/ thrombus, prosthetic heart valve, cardiac tumors = myxoma, paradoxical embolus from PFO, peripheral arterial/aortic atherosclerotic plaque embolism, aortic/artial aneurysms c/ embolism -Common femoral = #1 site of peripheral obstruction from emboli -Tx: embolectomy Need to return pulses . Post-op angiogram -Fasciotomy if >4-6 hrs ischemia (when permanent muscle + nerve damage begins, can get compartment syn 2/2 reperfusion) -Aortoiliac emboli (loss pulses in both feet) can be treated c/ bilat femoral artery cutdowns + bilateral embolectomies |
|
|
lower extremity compartment syndrome is defined by compartment pressure > _mm Hg
-most likely compartment = _ |
Acute arterial embolism:
-If >4-6 hrs of ischemia, do prophylactic fasciotomy to prevent compartment syndrome 2/2 reperfusion injury (permanent muscle, nerve damage begins @ 4-6 hrs) -Compartment pressure >20-30 mmHg is suggestive of compartment syndrome -Anterior compartment most likely => footdrop |
|
|
50M c/ no hx PVD develops cold painful R leg after missing warfarin for his A fib. LLE normal
-Tx is _ -Prophylactic fasciotomy would be indicated if.. |
EMBOLECOTOMY for acute arterial embolus
-Consider prophylactic fasciotomy, esp. if occlusion time >4-6 hrs |
|
|
Pt is 4 hrs post-op after embolectomy for acute arterial thrombosis, develops swollen, painful leg.
Next step _ |
Acute arterial embolism:
-If >4-6 hrs of ischemia, do prophylactic fasciotomy to prevent compartment syndrome 2/2 reperfusion injury (permanent muscle, nerve damage begins @ 4-6 hrs) -Compartment pressure >20-30 mmHg is suggestive of compartment syndrome -Anterior compartment most likely => footdrop |
|
|
Pt w/ hx fem-pop bypass presents c/ cool, mildly painful leg that does not look threatened
Next step = _ |
Acute extremity thrombosis, limb not treatened => angiography + thrombolytics
-Leg treatened => heparin + OR for thrombectomy -Thrombosed PTFE graft: limb not threatened => thrombolytics and anticoag. Limb threatened => heparin + OR for thrombectomy |
|
|
A 30 year old female presents with claudication of the right calf, but normal distal pulses. A CT angiogram shows a cystic filling defect in the popliteal artery. How do you proceed next?
|
Perform operative resection to remove cyst from the adventia. This patient has adventitial cystic disease, an uncommon cause of claudication that can lead to thrombosis and embolism. The cyst is found beneath the adventitia. Angiogram is diagnostic and helps identify both thrombus and emboli. Cyst aspiration or transluminal angioplasty are not advised while operative evacuation of the cyst cures the condition.
|
|
|
A 26 year old female presents with anorexia, myalgia, hypertension and cold ischemic left arm. An angiogram is done that shows multiple stenosis in the subclavian artery. What is true about the management of this patient?
|
The preferred treatment is high dose of steroids. The patient’s presentation is more suggestive of Takayasu arteritis. This young lady presenting with acute symptoms should be initially treated with daily high dose steroids. If she does not respond or if she relapses, she should be tried with additional treatment using methotrexate, cyclosporine, mycophenolate or infliximab. Once the acute phase is over, she may proceed with surgical treatment of symptomatic stenotic or occlusive disease. This can be achieved by percutaneous angioplasty or stenting or, in severe cases, by resection and placement of a prosthetic graft. This condition does not involve the coronary arteries. An endarterectomy is not recommended because of a high incidence of early failure.
|
|
|
What is hemodynamic contribution to aneurysm expansion and rupture?
|
Increased internal radius increases mean tensile stress . According to the Laplace law, both increased arterial blood pressure and increased internal radius are directly proportional to tensile wall stress, whereas aneurysm wall thickness is inversely proportional to wall stress. As a result, a 6 cm aneurysm arising from a 3 cm aorta has substantially less stress associated with it than the 6 cm aneurysm arising from a 1cm aorta.
|
|
|
what factors (think physics) are related to aneurysm rupture?
|
related to aneurysm rupture:
-thickness of aneurysm wall -arterial BP -internal diameter of aneurysm -radius of aneurysm (not flow rate) |
|
|
The anterior spinal artery syndrome is seen when someone suffers_
|
Transection of the thoracic aorta
|
|
|
What is the form of a peripheal arterial flow wave?
|
The Doppler signals have characteristic triphasic audible phases - early systolic rapid acceleration, a sharp peak at maximal velocity a rapid deceleration phase, a short flow reversal phase in early diastole caused by elastic recoil, and low-level forward flow through the remainder of diastole. Beyond an obstruction, the flow pulse becomes more rounded, the acceleration phase is less rapid, the peak is less well defined, the reverse flow component disappears, and the velocities remain above baseline throughout diastole.
|
|
|
patient on oral contraceptives presents c/ RUQ pain, hepatosplenomegaly, asites,elevated LFTs,
-Consider diagosis of _ -2 diagnostic modalities -Tx = _ |
Budd-Chiari:
-occlusion of hepatic veins + IVC -RUQ pain, hepatosplenomegaly, ascites, fulminant hepatic failure, muscle wasting, variceal bleeding -Dx: angio, CT. Liver bx: sinusoidal dilatation, congestion, centrilobular congestion. -Tx: portacaval shunt needs to connect to IVC above obstruction) |
|
|
_ = excellent method for monitoring bypass grafts
|
Duplex scanning is an excellent way to monitor bypass grafts. It can help detect graft-threatening defects before the patient has symptoms and before the ankle pressure begins to drop. A localized increase in systolic velocity greater than 100% of that of the adjacent graft identifies a diameter reduction of more than 50%. Peak systolic velocities less than 40 cm/s are an ominous sign of markedly reduced flow. Arteriovenous fistulas are regularly recognized by their pattern of localized flow disturbances. Velocities are high at the site of the fistula and immediately proximal to the fistula and concomitantly low just distal to the fistula.
|
|
|
51 yo male presents with ischemic right lower extremity. A femoral cutdown is performed and the embolus removed. Pathologic examination reveals spindle cells and primitive connective tissue in tissue sections. Which is the likely source of embolus?"
|
Cardiac myxoma
Common sources of arterial emboli include atrial fibrilation (50%), MI (25%), aneurysmal disease (6%), proximal artery (3%) and paradoxical emboli. Rare forms of intracardiac source include intracardiac tumors (atrial myxomas). |
|
|
Six months following carotid endarterectomy, a 72 year old female is seen in the emergency room for a painful lump in her neck on the side of her surgery. Physical exam reveals a painful, pulsatile mass. What is this?
|
Pseudoaneurysm of the carotid artery after CEA occurs following approximately 1/200 procedures. Presentation is typically 6 months following CEA and may involve a pulsatile neck mass, TIA secondary to microemboli, or voice hoarseness due to vagus nerve compression. Diagnosis is confirmed with duplex imaging and angiography is not necessary. Operative treatment is always indicated. Endovascular therapy, while theoretically possible with usage of a covered stent, is currently experimental for carotid pseudoaneurysm and cannot be recommended at this time. Further, a tender mass is concerning for an infected pseudoaneurysm which should not be treated with endovascular methods using prosthesis. Surgery should involve either closure (for small defects), or aneurysm excision and patch angioplasty, or exclusion and bypass when the carotid bifurcation is obliterated. The internal carotid flow must be re-established as ligation is associated with an high stroke rate (20-30%). Any suspicion of pseudoaneurysm infection warrants tissue culture and mandates avoiding prosthetic material use in vascular reconstruction.
|
|
|
CEA: 3 indications
|
Carotid endarterectomy (CEA)
->70% stenosis + sx OR >80% stenosis -Recent stroke => wait 4-6 weeks (less bleeding risk), then assess need -Emergent CEA for fluctuating neuro sx or crescendo/evolving TIAs -Shunt during CEA for stump pressures <50 -Repair tightest side 1st for bilateral stenosis, or dominant side first if stenosis is symmetric |
|
|
CEA pt, 2 hrs post-op develops neuro deficit in PACU.
Next step = _ |
CEA complications:
-20% get post-op HTN 2/2 carotid body injury => Nipride to avoid bleeding -Acute event immediately post-op => return to OR to eval for flap, thrombosis, hematoma -Psedoaneurysm: pulsatile bleeding mass after CEA => drape + prep, then intubate, then repair -MI = #1 non-stroke complication following CEA -15% restenosis rate |
|
|
how is HTN treated in the post-op period following CEA?
|
CEA complications:
-20% get post-op HTN 2/2 carotid body injury => Nipride to avoid bleeding -Acute event immediately post-op => return to OR to eval for flap, thrombosis, hematoma -Psedoaneurysm: pulsatile bleeding mass after CEA => drape + prep, then intubate, then repair -MI = #1 non-stroke complication following CEA -15% restenosis rate |
|
|
Pt develops a pulsatile, bleeding mass after CEA.
-Suspect _ -Tx is _ |
CEA complications:
-20% get post-op HTN 2/2 carotid body injury => Nipride to avoid bleeding -Acute event immediately post-op => return to OR to eval for flap, thrombosis, hematoma -Psedoaneurysm: pulsatile bleeding mass after CEA => drape + prep, then intubate, then repair -MI = #1 non-stroke complication following CEA -15% restenosis rate |
|
|
What is the msot commonly injured cranial nerve during CEA?
|
CEA anatomy;
-VAGUS = #1 cranial nerve injury - injury 2/2 vascular clamping -> hoarseness (RLN hasn't branched off yet) -Hypoglossal: tongue deviates toward injury, speech + chewing difficulty -Glossopharyngeal: only c/ very high carotid lesions -> swallowing difficulty -Ansa cervicalis: strap muscles, no serious defects -Mandibular branch of fascial nerve: corner of mouth (smile) |
|
|
Indications for CEA
|
Carotid endarterectomy (CEA) indications:
->70% stenosis + sx ->80% stenosis -Wait 4-6 weeks after any stroke 2/2 bleeding risk -Emergent CEA for fluctuating neuro sx or crescendo/evolving TIA |
|
|
Pt develops neuro deficit in PACU after CEA.
Next step is … |
Acute event immediately following CE ->
return to OR emergently to eval for flap, thrombosis @ suture line, hematoma compressing carotid, or some other reason which could cause neuro deficit |
|
|
Shunt during CEA if stump pressure <_
|
Shunt during CEA if stump pressure <50
|
|
|
Patient s/p CEA is hoarse.
Suspect _ |
Vagus = #1 cranial nerve injury c/ CEA
-Secondary to vascular clamping during endarterectomy -Get hoarseness Because recurrent laryngeal nerve has not branched off the vagus nerve at this level, injury to the vagus in the neck places the pt at risk for hoarseness |
|
|
A 65 year old male smoker experiences crampy pain in the calf bilaterally when walking two blocks. The pain is relieved when she stops walking. What dynamic change with regard to his ABI is expected when he exercises?
|
Resting ABI will be <1, then decrease during exercise.
The ankle brachial index (ABI) measures the ratio of systolic blood pressure at the pedal vessel (ankle) level relative to the brachial (arm) level. A normal ABI is 1.0-1.2. Patients with claudication, such as this patient, typically will have a decreased resting ABI in the 0.5-0.8 level. Rest pain is typically associated with an ABI less than 0.4 Exercise results in a further decrease in the ABI due to compensatory attempts at vasodilation in the affected leg. The consequence is decreased blood pressure at the ankle due to the combination of proximal stenosis and distal vasodilation. |
|
|
In a fasciotomy performed for leg compartment syndrome injury to which structure is most likely.
|

common peroneal nerve is the most commonly injured structure during leg fasciotomy
|
|
|
A 66 year old male with acute left lower extremity below knee popliteal artery occlusion due to a cardiac atheroemboli is seen emergently. He undergoes successful fogarty catheter embolectomy and has a normal completion angiogram. Two hours following the procedure the patient is complaining of left foot pain and numbness. Physical exam reveals : 1) palpable but deminished DP and PT pulses 2) a swollen calf 3) pain in the calf with dorsiflexion of the foot 4) subjective decreased sensation medial to the base of the great toe. The correct intervention is :
|
4-compartment fasciotomy
The muscle compartments of the below knee leg are anterior (housing the peroneal nerve inducing numbness at the first toe webspace), lateral, superficial posterior, and deep posterior compartments. Reperfusion injury occurs due to 1) microvascular capillary injury and interstitial leakage from the ischemic duration and 2)free oxygen radicals induced tissue damage and edema. These free radicals induce lipid peroxidation altering cell membranes, rendering them incompetent. |
|
|
Compartment syndrome:
-Suggested by compartment pressure > _ mmHg |
Compartment syndrome:
-Suggested by compartment pressure > 20 mmHg -May do prophylactic fasciotomy to prevent reperfusion-related CS in an extremity after embolectomy |
|
|
3 congenital conditions that predispose to aortic dissection
|
Cystic medial necrosis is associated with causing aortic dissection at an early age. It can be caused by Marfan's syndrome (type I collagen disorder) or type IV Ehlers Danlos syndrome, in which type III collagen is not produced. Patients with arteria magna syndrome have no elastic tissue in the media and an associated coronary artery disease is common, which may also predispose to dissection. However, in pseudoxanthoma elasticum, the elastic tissue is present in the media but it is replaced by calcific deposits. Patients may also have xanthoma like cutaneous papules.
|
|
|
Pt c/ hx A fib presents c/ colf painful leg after running out of Coumadin.
-Next step = _ |
Pt c/ hx A fib presents c/ colf painful leg after running out of Coumadin.
-Next step = EMBOLECTOMY +/- prophylactic fasciotomy to prevent reperfusion-related compartment syndrome |
|
|
Fibromuscular dysplasia (FMD) most commonly affects which arteries?
|
Fibromuscular dyplasia is an autosomal dominant disorder that most frequently affects the renal arteries. It involves fibrous thickening of the intima, media, or adventitia of arteries. In the renal arteries, FMD produces renal artery stenosis and can be a cause of refractory hypertension secondary to chronic upregulation of the rennin-angiotensin system. FMD tends to respond well to percutaneous balloon angioplasty, and this is considered first line treatment. After the renal arteries, the next most commonly affected arteries are the carotids, followed by the abdominal visceral arteries.
|
|
|
young women presents c/ HTN, no known cause
-must r/o _ |
Fibromuscular dysplasia:
-young women. -R renal artery most likely involved. -amenable to angioplasty |
|
|
A 19 yo female presents to regional trauma center 20 minutes after blunt injury to the right leg. Right lower extremity x-ray shows tibial plateau complex fracture and lack of pulses on the right foot. Next step in management include:
|
arteriography and operative exploration
Any pulse deficit in the setting of combined vascular and orthopedic injury warrants formal arteriography. Prolong or severe ischemia mandates immediate operative exploration. Direct arterial exploration is also warranted in open fractures. |
|
|
What is Griffith's point?
|
Griffith's point = splenic flexure:
-Junction of coverage by SMA and IMA = watershed area |
|
|
3 are used to treat homocysteinuria?
|
Homocysteinuria tx: folate, B6, B12
|
|
|
Two days following an open AAA repair, a 66 year old male experiences left lower quadrant abdominal pain and has three bloody bowel movements. He has a marked leukocytosis (wbc=21,000) with a bandemia on manual differential. What should be the next step in treatment?
|
"EMERGENT COLONOSCOPY to eval for ischemic colitis in IMA distribution = splenic flexure to superior rectum
(rest of rectum spared b/c inf + middle rectals come off int iliac). Colonoscopy can confirm. => mucosal hemorrhage, sloughing in sigmoid colon. -If transmural necrosis => laparotomy + resection of irreversibly ischemic bowel. -complication 2/2 inadequate collateral flow to IMA distribution + patent IMA artery at the time of aneursym repair. -no need to reimplant IMA if brisk back-bleeding from the IMA is encountered upon opening the aneurysm sac, -reimplant IMA if only small amount of back bleeding is encountered -Aorto-enteric fistula = late complication of AAA repair. Fistulization is typically to the duodenum. Peri-graft or retroperitoneal infection/inflammation = nidus for fistula |
|
|
_-type vessels don't have basement membrane
-(not found in bone, tendon, muscle, cartilage, brain, or cornea) |
Lymphatics;
-don't have basement membrane -not found in bone, tendon, muscle, cartilage, brain, or cornea |
|
|
patient taken urgently for angiogram for mesenteric ischemia has following findings:
-meniscus sign 5 cm from take-off of SMA -Jejeunal branches proximal to this normal -Diagnosis is most likely _ -Mgmt is _ |
SMA embolus:
-#1 site = near origin of SMA #1 source = heart -Pain out of proportion to exam, sudden onset, hematochezia -> peritoneal signs = late finding -Angiogram: meniscus sign, sparing of porximal jejunal branches (alternative: ab CT c/ contrast) 'RFs: a fib, endocarditis, recent MI, recent angiography -Tx: volume resuscitation, abx, open EMBOLECTOMY, resect infarcted bowel, heparin. 2nd look operation next day -TPA does NOT usually work for embolism |
|
|
patient taken urgently for angiogram for mesenteric ischemia has following findings:
-proximal narrowing @ take-off of SMA -Involvement of proximal jejunal vessels -Celiac occluded -Diagnosis is most likely _ -Mgmt is _ |
SMA thrombosis:
-Angiogram: 2 vessel disease, narrowing @ take-off of SMA (alternative: CT abdomen c/ contrast) -Usually c/ chronic food fear 2/2 mesenteric ischemia, weight loss -+/- hx of vasculitis or hypercoagulable state -Sx: similar to embolism, may have developed some collaterals -Tx: SMA thrombectomy, resection of necrotic bowel, usually needs SMA bypass 2nd look the next day. - NO peritoneal signs or melena => try catheter directed THROMBOLYTICS |
|
|
Pt has mesenteric ischemia.
What is the most common cause? What is the diffrerence b/w treatment approaches for embolism vs. thrombosis? |
Mesenteric ischemia:
-Mortality 50-70% -Ab CT: bowel wall thickening, intramural gas, portal venous gas, vascular occlusion -Acute embolism 50% > Thrombus 25% > Low flow state 15% > Venous throbosis 5% -SMA Embolism => volume resuscitation, abx, open EMBOLECTOMY (TPA usually doesn't work), resect infarcted bowel, heparin -SMA thrombosis => angiogram + TPA THROMBECTOMY , usually need SMA bypass (use angiogram info to map out bypass), resect infarced bowel, heparin -Mesenteric vein thrombosis => heparin, THROMBOLYTICS, can try mesenteric vein thrombectomy if diagnosed early, resect infarcted bowel |
|
|
NASCET study demonstrated that CEA reduces stroke rate from 26% to 9% if >__% stenosis
|
North American Symptomatic Carotid Endarterectomy Trial (NASCET) 1991:
pts under 80 y/o with 70%-99% symptomatic stenosis by CA. -All had experienced a hemispheric TIA, amaurosis fugax, or a nondisabling stroke in previous 4 months. The participants received antiplatelet therapy (usually aspirin) and were randomly assigned to either medical therapy alone (331 persons), or medical therapy plus CEA (320 persons). CEA was performed by either a vascular or neurosurgeon. At 2 years, the ipsilateral stroke (strokes occurring on the same side of the brain as the carotid stenosis) rate (26%) in the medical therapy group was significantly greater than the ipsilateral stroke rate (9%) of those persons receiving both medical therapy plus surgery. The overall average risk reduction of stroke was a significant 17% |
|
|
Pt c/ hx PVD, Afib off anticoagulation, on levophed and vasopressin for vasodilatory shock develops abdominal distenson, guiac (+) stools, leukocytosis, lactic acidosis.
Suspect _ 1st step _ |
Non-occlusive mesenteric ischemia (NOMI):
2/2 spasm, low-flow states, hypovolemia, hemoconcentration, digoxin -> final common pathway of low cardiac output state to visceral vessels -RFs: prolonged shock, CHF, prolonged cardiopulmonary vessels -Presentation: bloody diarrhea, pain -Watershed areas most vulnerable = Griffith's point, Sudak's point -Dx: Arteriogram -Tx: volume resuscitation, glucagon, paraverine, nitrates to increase visceral blood flow -Intra-arterial infusion of papaverine or nitroglycerine directly into culprit vessel -If angiogram shows embolus, can do open embolectomy (TPA doesn't usually work well for an embolus) -If thrombosis, can do thrombolysis c/ TPA, map for possible future bypass -Also need to increase cardiac output, resect infarcted bowel if (+) peritoneal signs |
|
|
The ophthalmic artery arises from the _
|
The ophthalmic artery arises from the internal carotid
|
|
|
Man presents c/ effort-induced thrombosis of subclavian vein.
Arm pain and swelling increases with activity, decreases with rest. What is this disease called? |
Pager-von Schrotter disease:
-Effort-induced thrombosis of SCV -Venous thrombosis >> Arterial -80% have associated thoracic outlet syndrome -Dx: venography = gold standard -Presentation: male, pain and swelling increased with activity, decreased with rest -Tx: THROMBOLYTICS, HEPARIN, WARFARIN, -> may eventually need operation for thoracic outlet syndrome if persistant sx (1st rib resection) |
|
|
_ = a xanthine derivative that is used to treat intermittent claudication resulting from obstructed arteries in the limbs, and vascular dementia
|
pentoxifylline = Trental
= a xanthine derivative that is used to treat intermittent claudication resulting from obstructed arteries in the limbs, and vascular dementia |
|
|
A 70 yr old woman with COPD is asymptomatic. She has a planned CT scan of the abdomen to follow up on an adrenal incidentaloma discovered 6 months ago. The CT reveals extensive pneumatosis intestinalis. What is the appropriate management?
|
OBSERVATION. Pneumatosis intestinalis, or gas within the bowel wall, is most commonly an ominous sign associated with ischemic or necrotic bowel. However, bowel ischemia presents with severe abdominal pain and peritonitis. The patient in the question above has none of these symptoms. Pneumatosis has less common causes, including COPD, bowel obstruction, and scleroderma. In the absence of peritonitis, laparoscopy or laparotomy are not indicated. Observation would be the most prudent course of action here.
|
|
|
What is the most common acute complication of popliteal aneurysm?
|
Popliteal aneurysms are the most common peripheral aneurysms (70%), followed by femoral aneurysms. 50% bilateral and 35% with AAA. Emboli and distal occulusion is the most common complication of true peripheral aneurysms (40% OF popliteal aneurysms). Rupture is rare.
|
|
|
Pt has prominent popliteal pulses, found to have 2.5 cm popliteal aneurysm on US.
-Most common complication is _ -Tx is _ |
Popliteal artery aneurysm:
-#1 peripheral aneurysm -Leg exam: prominent popliteal pulses -1/2 bilateral, 1/2 have another aneurysm elsewhere (AAA, femoral, etc.) 1/3 have AAA -Most likely to get limb ischemia 2/2 embolization > thrombosis (aneurysms below inguinal ligament rarely rupture) -Can also get leg pain 2/2 compression of adjacent structures -Surgical indications: symptomatic, >2cm, mycotic -Dx: US -Tx: exclusion + bypass. 25% of complication requiring amputation if not treated |
|
|
A 22 year old female is struck by an automobile and suffers an obvious dislocation of the right knee. She has palpable pulses in the right foot. There is no large hematoma at the knee. Evaluation should include"
|
Patients with posterior dislocation of the knee must be thoroughly evaluated to rule out popliteal artery injury. Up to 30% of patients with knee dislocation suffer arterial injury. Clues on physical exam to a possible arterial disruption are : deminished pulses or ABI on physical exam; large hematoma; cool extremity. If the patient is stable, angiography of the affected extremity is indicated. Orthopaedic consultation is appropriate after plain films of extremity are obtained. In the absence of hemodynamic instability, obvious arterial bleeding, or a rapidly expanding hematoma emergent surgical exploration is not indicated. Angiography allows better planning of the appropriate surgical intervention.
|
|
|
A 60 year old lady is found to have a 70% irregular stenotic lesion in the right carotid artery after being investigated for a TIA. She has a history of radiation to the right side of the neck a few years ago for a carcinoma. How do you proceed?
|
Radiation to the arteries can produce injuries as follows. The initial early injury after treatment consists of an inflammatory reaction with endothelial sloughing and thrombosis. Later, the fibrosis sets in and changes in the wall may produce stenosis or accelerated atherosclerosis. The atherosclerotic plaque is treated with standard endarterectomy, and the plaque itself is indistinguishable from non-radiated plaque.Patient has radiation induced arterial injury, which should be also treated with standard endarterectomy .
|
|
|
what is the course of the right renal artery?
|
R renal artery arises from aorta, passes POSTERIOR to IVC/renal vein as it courses to the kidney
|
|
|
Pt has signs/sx of mesenteric ischemia. Angiogram shows meniscus sign 5 cm below take-off of SMA, but jejeunal branches proximal to it are normal.
Ischemia is therefore likely 2/2 _ |
SMA embolus:
-#1 site = near origin of SMA #1 source = heart -Pain out of proportion to exam, sudden onset, hematochezia -> peritoneal signs = late finding -Angiogram: meniscus sign, sparing of porximal jejunal branches (alternative: ab CT c/ contrast) 'RFs: a fib, endocarditis, recent MI, recent angiography -Tx: volume resuscitation, abx, open EMBOLECTOMY, resect infarcted bowel, heparin. 2nd look operation next day -TPA does NOT usually work for embolism |
|
|
Pt has signs/sx of mesenteric ischemia. Angiogram shows proximal narrowing at take-off of SMA with involvement of proximal jejeunal vessels, celiac artery also occluded.
Ischemia is therefore likely 2/2 _ |
SMA thrombosis:
-Angiogram: 2 vessel disease, narrowing @ take-off of SMA (alternative: CT abdomen c/ contrast) -Usually c/ chronic food fear 2/2 mesenteric ischemia, weight loss -+/- hx of vasculitis or hypercoagulable state -Sx: similar to embolism, may have developed some collaterals -Tx: heparin, THROMBOLYTICS, mesenteric vein thrombectomy if diagnosed early, resection of infarcted bowel - NO peritoneal signs or melena => catheter directed thrombolytic tx -YES peritoneal signs => SMA thrombectomy, resection of necrotic bowel, SMA bypass, 2nd look the next day |
|
|
A 24-year-old female presents with RLQ abdominal pain. A CT scan confirms nonperforated appendicitis. There is an incidental finding of a 2.5 cm splenic artery aneurysm noted on the CT scan. The patient undergoes an uneventful appendectomy, and is discharged to home. On follow-up visit, she feels well, and does report that she and her husband would like to start a family when she recovers. The best advice to give about the splenic artery aneurysm is:
|
About 400 cases of ruptured splenic artery aneurysms are in the literature. About 100 of these cases occurred in pregnant women with a maternal mortality rate of 75% and fetal mortality rate >90%. When treated electively, the mortality is 0.5-1.3%. When the diagnosis of splenic artery aneurysm >2cm is made in a women of childbearing age, it should be treated surgically due to the catastrophic consequences of a rupture.
|
|
|
_ = #1 cause of splenic vein thrombosis
|
PANCREATITIS
Vascular complications of chronic pancreatitis are fortunately infrequent, because they are difficult to treat successfully. Portal vein compression and occlusion can occur as a consequence of an inflammatory mass in the head of the pancreas, and splenic vein thrombosis occurs in association with chronic pancreatitis in 4 to 8% of cases. Variceal formation can occur as a consequence of either portal or splenic venous occlusion, and splenic vein thrombosis with gastric variceal formation is referred to as left-sided or sinistral portal hypertension. Although bleeding complications are infrequent, the mortality risk of bleeding exceeds 20%. When gastroesophageal varices are caused by splenic vein thrombosis, the addition of splenectomy to prevent variceal hemorrhage is prudent when surgery is otherwise indicated to correct other problems |
|
|
A 60 year old man presents with sudden pain and ischemic changes in his right foot. An arterial embolus is suspected.
What is the annual risk of stroke c/ a fib? |
The annual risk of stroke with atral fibrillation is nearly 5% . 80% of arterial emboli originate in the heart, and 65% are caused by atrial fibrillation (A. fib). Chronic A. fib carries an annual risk of 3% to 6% for embolic complications while paroxysmal AF has a comparatively lower risk. Ischemic heart disease is the most common cause of chronic A. fib. Patients with A. fib on coumadin therapy have been found to have significantly reduced risk of stroke and other complications.
|
|
|
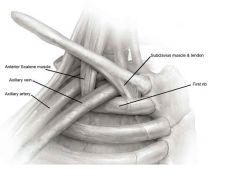
where is the subclavian artery located?
|
The structures of the lateral neck from anterior to posterior are:
Subclavian Vein, Phrenic Nerve, Ant. Scalene, Subclavian Artery, Brachial Plexus, Middle Scalene, Long Thoracic nerve, Posterior Scalene |
|
|
What is Sudak's point?
|
Sudak's point = rectum
-Junction of coverage by superior rectal and middle rectal arteries = watershed area |
|
|
53yr old steel mill worker who presents to the Emergency Room with a right arm redness, rash, and Horner’s syndrome should have what test ordered?
|
CT chest. This patient is presenting with SVC compression with associated Horner Syndrome. These are classically associated with an apical lung neoplasm, known as as a Pancoast Tumor. Pancoast lesions generally occur in the superior lung sulcus causing impingment on the sympathetic chain with SVC compression. Horner’s Syndrome, aka: oculosympathetic palsy, is defined by: pitosis, meiosis, ipsilateral anhidrosis, enopthalmos.
|
|
|
A 56 year old female experiences lightheadedness when peeling potatoes. When she stops using her right arm, the symptoms rapidly resolve. Extensive workup reveals a stenosed artery. Where is the anatomical location of the stenosis?
|
Right subclavian artery proximal to the vertebral artery
|
|
|
What is the most common anatomic abnormality causing thoracic outlet syn?
Most common presentation? |
Thoracic outlet syndrome:
-Normal anatomy: Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -#1 anatomic abnormality = CERVICAL RIB -Sx: NEURO (brachial plexus)> vascular sx affecting the back and neck. -Adson's test: turn head to ipsilateral side -> compresses SCA -> decreases radial pulse -Tinsel's test: tapping reproduces sx -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG |
|
|
Pt has cervical rib, presents c/ triceps weakness and atrophy, weakness of intrinsic hand muscles, weak wrist flexion.
What nerve is affected? C_-T_? |
Thoracic outlet syndrome:
-Normal anatomy: Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -#1 anatomic abnormality = CERVICAL RIB -Sx: NEURO (brachial plexus)> vascular sx affecting the back and neck. -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG -Radial distribution = superior brachial plexus: finger extensors, wrist extension -Ulnar distribution (C8-T1) = inferior brachial plexus: triceps weakness and atrophy, weakness of intrinsic hand muscles, weak wrist flexion Tx for brachial plexus sx = resection of cervical ribs, divide ANTERIOR SCALENES, middle scalenes, +/- 1st rib resection |
|
|
Pt has cervical rib, presents c/ weakness in finger extensors, wrist extensors.
What nerve is affected? |
Thoracic outlet syndrome:
-Normal anatomy: Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -#1 anatomic abnormality = CERVICAL RIB -Sx: NEURO (brachial plexus)> vascular sx affecting the back and neck. -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG -Radial distribution = superior brachial plexus: finger extensors, wrist extension -Ulnar distribution (C8-T1) = inferior brachial plexus: triceps weakness and atrophy, weakness of intrinsic hand muscles, weak wrist flexion Tx for brachial plexus sx = resection of cervical ribs, divide ANTERIOR SCALENES, middle scalenes, +/- 1st rib resection |
|
|
Pt works as a pitcher, presents c/ funny arm symptoms.
Suspect _ (maximal arm abduction -> absent radial pulse) |
Thoracic outlet syndrome:
-Normal anatomy: Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -Pitchers can get annterior scalene hypertrophy -> SCA compression. (-) RADIAL PULSE WITH MAXIMAL ARM ABDUCTION. -Adson's test: turn head to ipsilateral side -> compresses SCA -> decreases radial pulse -Tinsel's test: tapping reproduces sx -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG Tx for PITCHERS: cervical rib + 1st rib resection, divide anterior scalenes, BYPASS GRAFT |
|
|
What is the rate of symptom resolution after surgery for thoracic outlet syndrome?
|
Thoracic outlet syndrome:
- 60% success rate (complete symptom resolution) after surgery for throacic outlet syndrome -Normal anatomy: Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -#1 anatomic abnormality = CERVICAL RIB -Sx: NEURO (brachial plexus)> vascular sx affecting the back and neck. -Adson's test: turn head to ipsilateral side -> compresses SCA -> decreases radial pulse -Tinsel's test: tapping reproduces sx -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG |
|
|
For a superior approach for thoracic outlet syndrome repair, where is the phrenic nerve
|
Thoracic outlet syndrome:
-Phrenic nerve is anterior to anterior scalene -Long thoracic nerve is posterior to middle scalene -Branchial plexus + SCA go through a triangle = superior to 1st rib, posterior to ant scalene, anterior to middle scalene. SCV also over 1st rib but anterior to ant scalene. -#1 anatomic abnormality = CERVICAL RIB -Sx: NEURO (brachial plexus)> vascular sx affecting the back and neck. -Adson's test: turn head to ipsilateral side -> compresses SCA -> decreases radial pulse -Tinsel's test: tapping reproduces sx -Dx: CXR, C spine x-ray, angiography if thought to be vascular etiology, EMG |
|
|
Which structure (layer) in the artery bears most of the tensile load?
|
Media. Amongst the different layers within the arterial wall, the intima compromises endothelial cells and internal elastic lamina. It provides minimal tensile strength. The media is primarily composed of collagen, elastin, and smooth muscle cells. It carries most of the tensile load. The adventitia is composed of fibrous connective tissue, vasa vasorum, and nerve fibers that regulate medial smooth muscle cell tone.
|
|
|
Splenic aneurysm:
-_% of all visceral aneurysms -3 indications for surgery |
Visceral aneurysms:>2 cm
-Splenic: 60%. 2% risk of rupture. Repair if >2 cm, childbearing age/planning pregnancy, or symptomatic -Repair all others b/c 50% risk of rupture. Exclusion + bypass graft. -Splenic and proximal common hepatic can just be excluded (have good collaterals) -RFs: medial fibrodyspaplsia, portal HTN, arterial disruption 2/2 inflammatory dz e.g. pancreatitis |