Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back

1.define Traumatic Spondylolithesis of Axis (Hangman's Fracture)
2. MCC hangman's fx, Associated injuries? 3 desc the mech of inj causing trauma |

1.Traumatic anterior spondylolithesis of the axis (c2) due to bilateral fracture of pars interarticularis
2 MVA, 30% assoc have concomitant c-spine fx 3. hyperexten->fracture of pars then flexion->tears PLL & disc allowing subluxation |
|

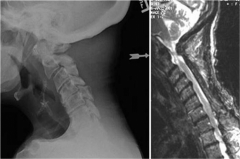
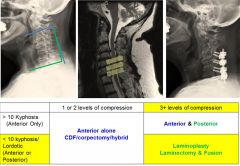
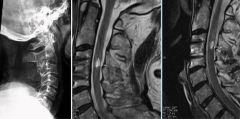
neutral lateral cervial radiographs and corresponding T2-weighted MRI of pts w/ sx & PE w/ cervical myelopathy. In which of these patients would a cervical laminoplasty alone be contraindicated as surgical treatment?
|
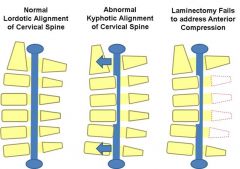
Laminoplasty alone as surgical tx is contradindicated in pts w/ rigid cervical kyphosis of > 13 degrees, obtaining flex/ext films, one can determine if the kyphotic deformity is rigid or not.
|
|

47yo F w/ T-2 DM & pacemaker c/o b/l buttock & leg pain that > w/ prolonged walking & improves w/ sittg. Her LE sx she feels "unstable" on her ft. PE= 5/5 in all muscles LE, (+) conus, lum myelo Fig. What is the next step in tx.1-Lum decomp; 2-Lum decomp w/ arthrodesis 3-trial of PT & NSAIDS; 4-Lum epidural steroid inj;5-CT myelogram C spine
|

myelopathy and neurogenic claudication in a pt w\ lum degen spondylolithesis. CT myelo C spine is next step in management, sx tandem stenosis can present w/ a confusing scenario of both neurogenic claudication and myelopathy. The prevalence has been estimated to be from 5% to 25%.Ans5
|
|

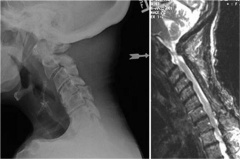
56yo F c/o- initial eval neck pain, which wosened by activity x many yrs. PE, 5/5 strength b/l UE & LE, nl gait, no diffi w/ manual dexterity, Reflex testing= hyperreflexia b/l achilles T. Lat xrays Fig A & MRI scan Fig B &C. What is management?
|

1-C4-7 ant decom w/ instrum fusn 2-C4-7 pos decom w/ instrum fusn; 3-C4-7 pos decom w/out fusn 4-C5/6 ant disc & fusn; 5-PT:::Minimal sx w/out hard evidence of gait disturbance or pathologic reflexes; nonop tx, PT.Ans5
|
|
Which variables has the strongest assoc w/ poor clinical outcomes in pts who undergo expansive laminoplasty for cerv spondylotic myelopathy? 1- Multi-level stenosis; 2-Duration of sx; 3- Local kyphosis > 13 deg; 4-Osteopor;5-MRI CSF effacemnt
|
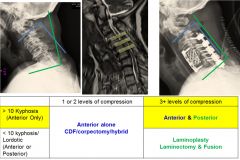
Fixed cervical kyphosis is assoc w/ poor func outcomes, kyphosis of > 13 degrees and signal intensity change on MRI were the most crucial risk factors for poor surgical outcomes.Ans3
|
|
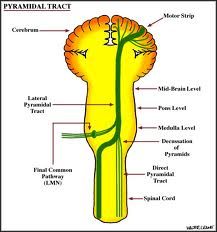
All are clinical signs and characteristic of an upper motor neuron disorder EXCEPT? 1-Fasciculations; 2- Spasticity; 3-Mus weakness 4-Exaggerated DTR 5- Sustained clonus
|
low motor neuron =nerve fibers traveling: ant horn of S.C. ->peripheral muscle, char= fasciculations & flaccid paralysis. Up motor neuron= nerve fibers traveling: motor cortex of brain -> ant horn of S.C., 4-char = spastic paralysis, exaggerated DTR, sustained clonus, up-going Babinski. Mus weakness is both uppr & lower MN.Ans1
|
|
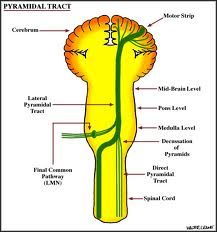
mnemic: for Lower vs. upper motor neuron lesion effects
|
"STORM, Baby"='In a Lower motor neuron lesion, everything goes Down: S-Strength; T-Tone; O-Other
R-Reflexes; M-Muscle mass; BABI-BABInski's sign In Lower all things go down: strength, tone, reflexes, muscle mass, and the big toe down in plantar reflex (Babinski's sign is big toe up: toe up = UMNL). |
|

Following a C3-C7 laminoplasty in a myelopathic pt w/cervical stenosis, the MC neurologic complicwould manifest with which new posteop exam findings? 1-Change in voice & diff swallowing; 2-Triceps weak; 3-Deviation tongue; 4-Ptosis, miosis, anhydrosis; 5-Biceps weak
|
A C5 palsy (motor-dominant type 1^deltoid &2^ biceps weak) is MC neurologic compl p/cer laminoplasty, incidence 5%. Its pathogenesis & prevention & tx remain unidentified & many controversies, 6-9 mth before recommending tx, nerve transfers w/brachial plexus injuries to restore func include:motor-dominant type
Triceps to axillary N transfer-> restore deltoid muscle, Double fascicular N transfer->restore elbow flex, Distal spinal accessory to suprascapular N transfer-> restore function in the supraspinatus & infraspinatus M.Ans5 |
|

pts w/sx of Cer myelopathy, what is asso w/ improved outcomes w/ nonop managt? 1-Inc Central Motor Cond Time (CMCT); 2-Transverse area spinal cord >70mm; 3- Isolated low intramed signal on T1WI; 4-midsagittal diameter of the spinal canal of <13mm 5-Younger age
|

most likely to be successful when there is a larger transverse area of the SC, They found pts w/ good outcomes w/ conserv tx were older in age, nl central motor conduction time (CMCT), and had a larger transverse area of the spinal cord (>70mm).Ans2
|
|
Postop radiculopathy is a known compl of pos cervical decompression for myelopathy. One potential mech of nerve root inj is thought to be tethering of nerve root w/dorsal migration of the SC. What is the MC radicular pattern seen?
|
1-Mot-dom radiculopathy w/ weak @ deltoid
2-Sen-dom radiculopathy w/ pain @ lat shoulder; 3-Mot-dom radiculopathy w/ weak @ wrist ext; 4-Sen-dom radiculopathy w/ pain @ lat forearm 5-Mot dom radiculopathy w/ weakness of the triceps:::motor-dominant type dletoid.Ans1 |
|
Which classification system for cervical myelopathy focuses exclusively on lower ext function? 1-Nurick; 2-Japanese Ortho Assoc; 3-Mod Japanese Orth Ass; 4- Ranawat; 5-Oswestry
|
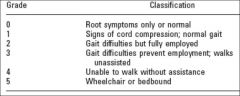
Nurick Classification sys focuses on the ambulatory status of the pt. jap Ortho Ass Class sx: chopstick func. Ranawat Class UE & LE sx, Oswestry Disability Index for back pain, not cervical myelopathy.Ans1
|
|

21yo college football player sustains transient loss of motor func in his arms after a collision. Which is an absolute contraindication to return to play? 1-Ant cervical diskectomy & fusion 1 level HNP; 2-Torg ratio < 0.8 w/ no neurologic sx; 3-Cord signal changes MRI ; 4-Frequent episodes of stingers when he was in high school; 5-Chronic neck & back pain
|
athletes multiple episodes of transient quadriparesis/ b/l ext sx w/MRI evidence of cord injury should be avoid, contact/collsn sports. It was found that the presence of an abn Torg ratio does NOT appear to be predictive of future spinal cord injury.Ans3
|