Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
6 Cards in this Set
- Front
- Back

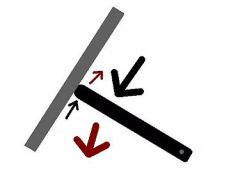
56yo M s/p1 yr p THA w/ the implant Fig A. He is concerned about the potential complctns. He is asymptmtc. Which is accurate re: prosthesis & future care? 1- bi-annual LFTs measrd, as metal ions metablzd by liver;
|

2-risk CA dramatically inc'd; 3-no corrltn bw/ activity & serum levels of metal ions; 4.prosthesis design safe in women of child-bearing age; 5-prosthesis design-> inc'd risk for dislctn::MOM THR activity level does NOT affect metal ion levels.Ans3
|
|

80 yo M has a Charnley all-poly acetabular shell Fig A. When def'g failure as revision for any reason, what is the failure rate at 35 years for this type of prosthesis? 1-<10%; 2-20%-30%; 3-40%-50%; 4-50%-75%; 5->75%
|

::77.3% survivorship for the component @ 21 yrs, w/ revision/definite loosening as an endpoint. 84% surviving @ 20 years without revision. there is a significantly inc'd probability of revision based on the age of the pt.Ans2
|
|

All are features: metal-on-metal THA allows for improved fluid film lubrication b/w compnts EXCEPT: 1-Largr fem hd; 2-Slight clearance of fit b/w acetblr cup & fem hd; 3-Min surfc roughns fem hd; 4-Complt congruence fit b/w acetblr
|

cup & fem hd; 5-Min surface roughness acetblr cup::Slight clearance, not complete congruence, is optimal. ideal fluid film lubrication regime minimizes friction. largr hd size > full-film lubrication.Ans4
|
|

All are true for pt who underwent a metal-on-metal (THA) EXCEPT? 1-they will have ionically chargd wear particles; 2-highr CA risk than with metal-on-poly THA; 3-elevtd levels Co & Cr in serum; 4-elevtd levels of Co & Cr in urine
|
5-highr frictional torque> ceramic on ceramic THA:: To date, there is NO correlation b/w metal serum levels & CA risk. metal-on-metal THA has > frictional torque than ceramic on ceramic THA.Ans2
|
|
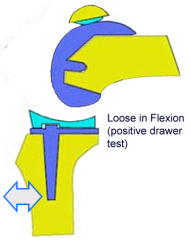
66yo M TKA w/ fixed bearg post stabiizd compnt. intraop trialg components: flex gap-loose & ext gap-appropriate. If this is not corrected, what post-operative complctn risk? 1-Spin out poly; 2-Periprosthtc fx;
|
3-Pos knee dislctn; 4-O-lysis; 5-Patellar instblty:: If knee is too loose-flex, possbl fem compnt "jump the post" grt pos dislctn. Tx-revision surgery only way to correct sx flex instability.Ans3
|
|

dur'g TKA trial; knee is stable at full extension, but it will not flex past 90 deg. Which adjustments can achieve satisfactory ROM & stability flex/ext? 1-Downsiz'g tib insert; 2-Placg pos fem augments; 3-Resectg more dis fem;
|
4--Downsiz'g fem compnt; 5-Performg medial tib reduction osteotomy::TKA >flexion, 5 options: 1downsizg fem compnt, 2recessg PCL, 3inc'g pos tib slope, 4 resectg more tib 5 decg ht tib insert;Ans4
|