![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
25 Cards in this Set
- Front
- Back
|
How are norms for ABR based?
|
on stimulis parameters (intensity, click rate, etc) |
|
|
know |
|
|
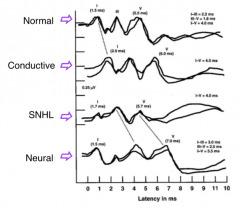
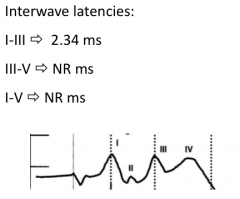
What are the general findings for ABRS in conductive losses and why? |
All waves are pro prolonged, including wave I, however interweave latencies are well within normal limits
this is because the conductive component reduces the stimulus intensity in the cochlea, however once it reaches the cochlea, a normal ABR is seen |
|
|
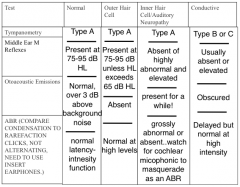
How does otitis media affect the ABR? |
|
|
|
What are the general findings in ABRs with HFSNHL? |
|
|
|
How is ABR affected by cochlear HL? |
Wave V latency & waveform morphology are progressively affected by
normal wave V latencies have been recorded in pts with
|
|
|
How is ABR affected by degree of cochlear HL? |
|
|
|
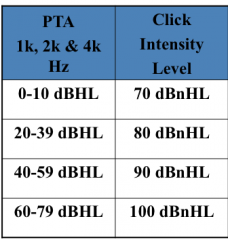
How should you modify the stimulus based on the amount of HL?
|
|
|
|
What is the general rule for modifying stimulus based on the amount of hl? |
present at least 20 dB higher than the threshold in the 2-4 kHz region |
|
|
What are some ways to increase wave I identification in cochlear HL? |
|
|
|
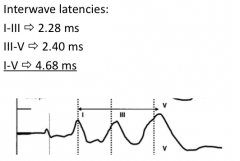
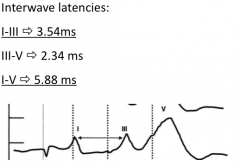
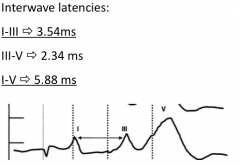
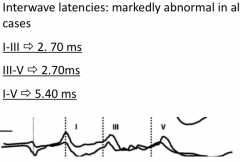
What are the general findings in ABRs with retrocochlear disorders and why? |
wave I is present with normal latencies, however there is a delay in latency between wave I-III
because the response is reflecting transmission of auditory signal along the VIII cranial verve |
|
|
What are possible occurrences with ABR and retrocochlear disorders? |
|
|
|
What are potential disorders associated with these retrocochlear findings? |
vestibular schannomas (aka, acoustic neuromas, neurinomas, neurilemmomas)
neoplasms (meningiomas and gliomas)
positive identification of large tumors (~2cm and up) - ~92-98% positive ID (small tumors often missed) |
|
|
So if the ABR doesn't catch the retrocochlear, what will? |
MRIs with Gd-DTPA - the gold standard in identifying cerebellopontine angle tumors
allows for ID of tumors as small as 0.3 cm x 0.3 cm |
|
|
abnormal ABRS may be seen in patients with what neurological disorders? |
|
|
|
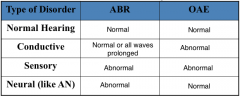
How is ABR in those with auditory neuropathy? |
puts display disorder at the level of inner hair cells and/or auditory nerve
typically bilateral
|
|
|
... |
|
|
... |
|
What should you consider when seeing this? |
|
|
What if this is a unilateral finding? |
characteristic of a TUMOR related to auditory dysfunction in the region of the VIII nerve or lower brainstem (cerebellopontine angle) |
|
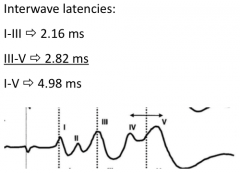
What if this is a bilateral finding? |
its a characteristic of brainstem (pons) dysfunction
less common of a bilateral VIII nerve dysfunction (neurofibromitosis) |
|
What could be going on here? |
|
|
What's going on here? |
|
|
What could be going on here? |
unusual occurrence
check patient characteristics and rerun |
|
What's going on here? |
sign of severe brainstem dysfunction
clear waves I and II rule out serious auditory problem |