![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
43 Cards in this Set
- Front
- Back
|
Risk factors for lung cancer |
smoking*** 90% (smokers 20x risk; dose effect)
weaker: smoking pipe, cigar, marijuana, cocaine
radiation
environmental: second hand smoke, asbestos, radon, Uranium, chemicals like formaldehyde
HIV infxn hx of lung cancer in family dietary factors (beta-carotene) controversial |
|
|
what if you smoke and have asbestos exposure? |
60x risk |
|
|
how does lung cancer present? |
weight loss chronic cough (3 wks+) (50-75%) hemoptysis chest pain hoarseness |
|
|
chronic cough is most frequently seen in what kind of cancer?
what other way does the cough happen? |
squamous cell and small cell carcinomas because those are in central airway locations
sometimes related to post-obstructive recurrent pneumonia
if it's a new cough in a smoker- raises suspicion |
|
|
hemoptysis: what percent of cancer pts have?
what's the most common cause of hemoptysis? |
25-50% of pts
bronchitis. So if hemoptysis without infective sx, do bronchoscopy |
|
|
chest pain: percent of cancer pts?
what is involved?
quality? |
20%
mediastinum, pleura, chest wall
dull, aching, non-resolving ipsilateral to cancer pleuritic pain: sharp if direct pleural metastasis, post obstructive pneumonia, PE |
|
|
hoarseness
dyspnea
wheezing |
laryngeal cancer or lung cancer
25% of pts, airway obstruction, pleural effusion, tamponade, emboli, atelectasis, pneumonia
unilateral wheezing raises suspicion of object or mass, so adult: mass |
|
|
when do pleural effusions happen? |
malignant pleural effusions- considered metastatic dz (Stage IV) and managed palliatively. Can get dyspnea or cough from this but 25% asx.
can also be from: lymphatic obstruction post-obstructive pneumonitis atelectasis |
|
|
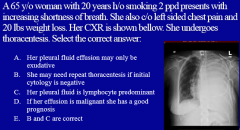
what are pleural effusions like in malignant effusion? what is the fluid like? |
exudative so high protein and/or high LDH lymphocytic predominant, sometimes high in eosinophils fluid varies: serous, serosanguineous, grossly bloody |
|
|
how to use malignant effusion to confirm tumor presence? |
single pleural fluid cytology is 60% 3 -> 85%
surgical thoracoscopy medical pleuroscopy |
|
|
sensation of fullness in head dyspnea cough pain dysphagia
dilated neck veins prominent venous pattern on chest facial edema plethroic appearance |
SVC syndrome |
|
|
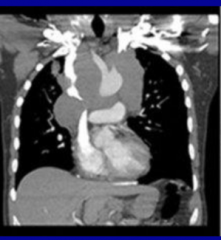
what is superior vena cava syndrome? |
obstruction of SVC from the tumor- more common in small cell
sx resolve after tx of mediastinal tumor |
|
|
SVC being compressed |
|
|
what happens if you have SVC syndrome pt lift arms? |
blood comes down and fills face/head |
|
|
pain in shoulder or forearm, scapula, fingers
ptosis myosis anhydrosis bony destruction atrophy of hand muscles |
Pancoast syndrome |
|
|
What is Horner's syndrome? |
ptosis myosis anhydrosis |
|
|
what usually is involved in Pancoast syndrome? |
non-small cell lung cancer so squamous cell cancer |
|
|
where are the common metastases of lung cancer |
liver: asx, elevated LFT's
bone: pain in back, chest, extremity, elevated serum alk phosphatase, osteoclastic
adrenal glands: asx
brain: headache, vomit, visual, hemiparesis, cranial nerve deficit, seizure |
|
|
what other issues are there during advanced cx presentation |
hypercalcemia SIADH (SCLC) neurologic (SCLC) hematologic cmplications: anemia, leukocytosis, thrombocytosis, hypercoagulable disorders hypertrophic osteoarthropathy Cushing's syndrome dermatomyositis and polymyositis |
|
|
hypercalcemia |
one metastasis/destruction, but sometimes PTH emitting tumor or calcitriol
sx: anorexia, nausea, constipation, polyuria, polydipsia, dehydration
tx: bisphosphonates and hydration |
|
|
SIADH |
syndrome of inappropriate antidiuretic hormone secretion- SCLC
causes hyponatremia
anorexia, nausea, cerebral edema
tx: cancer, fluid restriction, vasopressing- receptor antagonist |
|
|
neurologic |
SCLC often immune-mediated by autoantibodies includes Lambert-Eaton myassthenic syndrome LEMS |
|
|
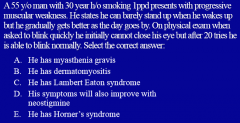
What is Lambert-Eaton myasthenic syndrome? |
SCLC auto antibodies against presynaptic Ca channels
symmetrical slow progressive proximal muscle weakness autonomic dysfunction CN involvement |
|
|
hematologic: hypercoagulable disorders |
Trousseau's syndrome: migratory superficial thrombophlebitis DVT and thromboembolism disseminated intravascular coagulopathy thrombotic microangiopathy nonthrombotic microangiopathy |
|
|
leukocytosis |
overproduction of granulocyte-CSF
eosinophilia rare
LCLC |
|
|
hypertrophic osteoarthropathy |
clubbing and periosteal proliferation of tubular bones- lung cancer and other lung dz
symmetrical painful arthropathy
often resolves after resection, or NSAID and bisphosphonate |
|
|
cushing's syndrome |
ectopic production of ACTH
muscle weakness wt loss htn hirsutism osteoporosis hypokalemic alkalosis hyperglycemia
SCLC |
|
|
dermatomysotitis and polymyositis |
muscle weakness heliotropic rash Gottron papules |
|
|
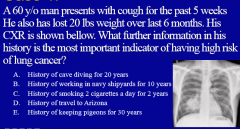
B: asbestos exposure
AZ is about coccidioides cave and pigeons for histoplasmosis |
|
|
C |
|
|
B and C so E
lymphocytic predominent, may have to do cytology 3 times.
bad px |
|
|
how to dx |
screening if high risk individual with CT
imaging: nodules or nodule
if intermediate risk: PET scan
if positive PET or high risk: biopsy |
|
|
what pts are high risk |
older smokers FHx of cancer hx of prior cancer occupational exposure |
|
|
evaluating nodules |
usually benign from infxn, autoimmune, pneumonconiosis
but if vary in size, pheripheral and at end of vascular bundles.. worried about metastasis |
|
|
evaluating a single nodule |
benign or malignant
depends on pts
size: larger the worse growth rate: faster worse, measure diameter edges: benign well-defined, irregular/spiculated is bad
calcification: dense central, laminated, popcorn, diffuse for benign. Eccentric/random is bad location- upper and middle lobe location |
|
|
what does the PET scan show? |
wmetabolic activity so positive in malignancy, inflam or infxn
better if above 8mm |
|
|
what are common false positives and false negatives for PET scans |
infxn, abscesses, RA nodules, sarcoidosis
caricinoid, well-differentiated, lymphoma, metastasis |
|
|
how all can you biopsy lung |
bronchoscopy: parenchymal and lymph
percutaneous CT guided Fine Needle Aspiration FNAo- higher pneumothorax risk, best for pleural based lesions
surgical biopsy: open lung |
|
|
left: SCLC
right: NSCLC |
|
|
what are the stage definitions |
Stage IA no invasion IB: main bronchus <5cm IIA: >5cm in main bronchus IIB if plus a lymph node or >7cm III: 2 lymph nodes. A: resectable. B not. (everything before can be cured with surgery) IV broke out |
|
|
SCLC px
tx |
poor
without tx 2-4 months
with tx 1.5 to 2 years
platinum (cisplatin, carboplatin) topoisomerase inhibitors (cytopenia, secondary cancer) |
|
|
C to see if there is a bigger mass or something, since the ab CT will only show part of it
(PET is only if it's bigger; first two are overkill) |
|
|
C
not surgery. Bad px. Can't just say go home. |