![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
77 Cards in this Set
- Front
- Back
|
Why is chest imaging nonspecific? |
-Radiologist sees varying density on radiograph or CT -Density could be blood, pus, water, or cells -Use associated findings and clinical history to give best guess at the cause of density |
|
|
Indications for conventional chest CT |
-Known or suspected malignancy -Pulmonary nodule evaluation -Trauma -Respiratory sx: cough, dyspnea (after CXR) -Chest pain |
|
|
Indications for high resolution chest CT |
-Evaluation of diffuse pulmonary disease, particularly interstitial lung disease -Suspected small and/or large airway disease - includes eval of bronchiectasis |
|
|
HRCT takes images during ____ |
expiration |
|
|
With high resolution chest CT, some structures at the level of the ____ are visible |
secondary pulmonary lobule |
|
|
CT angiography procedure |
iodinated contrast material injected IV contrast material "opacifies" the blood which then appears whiter on CT images |
|
|
Thoracic MRI indications |
-Chest wall tumors, vascular if can't get contrast, mediastinal invasion by tumor -Certain mediastinal masses/abnormalities -Cardiac abnormalities -Aortic disease when patients can't get contrast (allergy or renal failure) |
|
|
2 main types of pulmonary edema |
Hydrostatic Increased permeability |
|
|
Cardiogenic pulmonary edema |
LV failure --> inc L atrial pressure --> inc pulmonary venous pressure (hydrostatic Pulmonary edema) |
|
|
Increased pulmonary venous pressure also called... |
pulmonary venous HTN |
|
|
Early radiographic sign of decompensation is ____ |
redistribution or "cephalization" of flow - from lower zones to upper zones |
|
|
On a normal upright CXR, the pulmonary vessels are larger in the ____ than the ____ |
lower zones > upper zones |
|
|
Pulmonary edema is best assessed on _____. Why?
|
Upright CXR - especially PA CXR On AP supine CXR there is equalization of blood flow in upper, mid and lower zones |
|
|
Interstitial pulmonary edema |
-Pulmonary venous pressure increases --> fluid accumulates in the interstitium -Central (axial) + peripheral interstitium |
|

If R is normal, pathology on the L? |
L shows distended upper zone pulmonary vessels consistent with pulmonary edema |
|
|
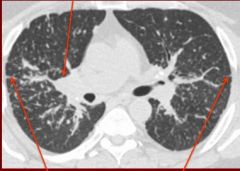
In interstitial pulmonary edema, where does the fluid initially accumulate? Other findings? |
-Central interstitium runs along the bronchovascular bundles -- edema fluid accumulates here first -Ill defined pulmonary vessels -Peribronchial cuffing |
|

Pathology on the R? |
Vessels are distended and their margins are ill-defined - pulmonary edema |
|
|
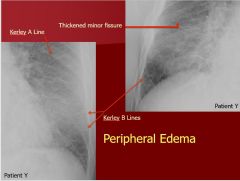
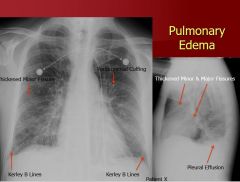
Secondary changes in pulmonary edema? |
-Peripheral interstitium extends along interlobular septa and subpleural margins -Kerley lines = thickened interlobular septa -Subpleural interstitial edema is manifested as fissural thickening |
|
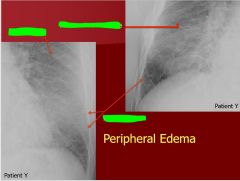
Pathologic findings? |
|
|
|
|
|
|
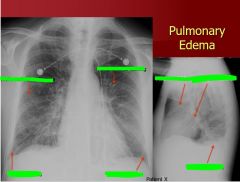
Final stage of pulmonary edema? |
Alveolar flooding - alveolar/air space edema |
|
|
Pulmonary capillary wedge pressure correlation with radiologic findings |
-5-12: normal findings -12-17: cephalization of pulmonary vessels (only in chronic conditions) -17-20: kerley lines, subpleural effusions (interstitial edema) ->25: pulmonary edema |
|
Pathology? |
Cardiogenic pulmonary edema - ground glass opacity ==> hazy density but still see normal lung architecture Arrow indicates Kerley line |
|
|
ARDS |
-Clinical syndrome -Type of permeability edema -Diffuse alveolar damage present histologically |
|
|
CXR findings for ARDS/diffuse alveolar damage |
-Early on the CXR may be normal or show interstitial edema or decreased lung volumes -Rapidly progresses to widespread air space consolidation -Progresses to fibrosis, traction, bronchiectasis, cysts |
|
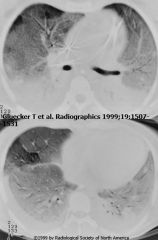
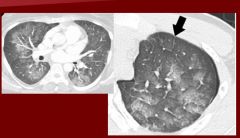
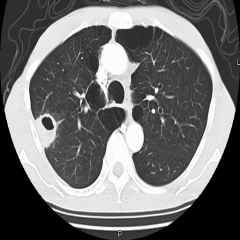
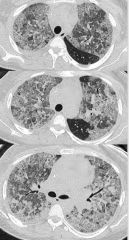
Findings? |
-CT demonstrates diffuse ground glass and consolidative + opacities that often are greater in dependent portions of the lung
|
|
|
As ARDS progresses _____ develops. This is manifested by ____ and ____. |
As ARDS progresses, fibrosis develops. This is manifested by traction bronchiectasis and intrapulmonary cysts. |
|
|
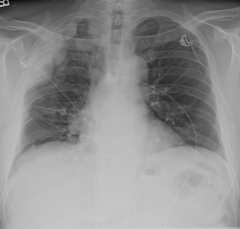
First imaging chest obtained for PE? |
CXR - often normal in pts with pulmonary emboli; no specific findings sufficient to confirm or exclude PE on CXR |
|
|
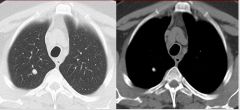
Westmark sign |
Oligemia (decreased vascularity and increased lucency) of a lung or portion of a lung distal to a pulmonary embolus (insert picture) |
|

Pathology? |
Westmark sign - oligemia (decreased vascularity and increased lucency) of a lung or a portion of lung distal to a pulmonary embolus |
|
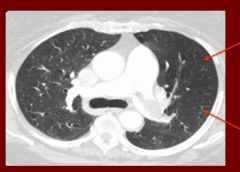
Pathology? |
Westmark sign - decreased vascularity in the lung affected by the PE |
|
|
Hamptom hump |
Circumscribed, subpleural opacity with a round medial border facing toward hilum (insert picture) May represent pulmonary hemorrhage without infarct or true pulmonary infarct |
|

Pathology? |
Hampton hump - circumscribed, subpleural opacity with a rounded medial border facing toward the hilum |
|
|
When are true pulmonary infarcts more likely? |
In pts with diminished cardiopulmonary reserve as both the pulmonary and bronchial artery systems are impaired |
|
|
PE associated finding? |
Estimated that over 80% of PE cases associated with DVT |
|
|
Pros of doppler venous ultrasound |
-No ionizing radiation -Rapid -Inexpensive -If positive patients are usually anticoagulated without need for further imaging -Debate whether or not it should be the first imaging test in pregnant patients suspected of having a PE due to the advantage of no ionizing radiation |
|
|
Cons of doppler venous ultrasound |
-Not always available after hours -May be negative in patients with PE, usually reserved for patients with symptoms of DVT |
|
|
V/Q scan for PE |
Normal perfusion pattern in multiple projections plus normal ventilation scan indicates that no pulmonary emboli are not present and no further workup necessary |
|
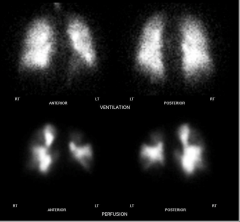
What does this vq scan indicate? |
Pulmonary embolism - ventilation is appropriate but perfusion is patchy, wedge shaped areas indicate segments of lung blocked off by PE |
|
|
CTPA for PE |
Gold standard -High accuracy -Low false negative rate -May occasionally demonstrate pathology other than PE as cause of pts sx (PNA, pulmonary edema, etc) |
|
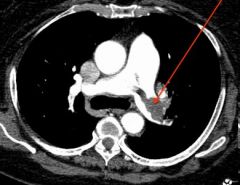
Pathology? |
Pulmonay embolus indicated by CTPA - portion of the pulmonary artery that contains the clot does not opacify with contrast so it appears as a darker filling defect |
|
|
CTPA may be nondiagnostic if _____ |
pt can't hold their breath |
|
|
Comparison of CTPA vs V/Q for pulmonary embolus |
1) CTPA: -Higher radiation dose -Requires IV contrast -May be nondiagnostic if patient can't hold breath -Often more definitive -May find other cause for symptoms 2) V/Q -Lower radiation dose -Can perform in patients with contraindications for IV contrast -Not impaired by respiratory motion -Not as readily available "after hours" -Less diagnostic in patients with abnormal CXRs |
|
|
What to do if suspected PE during pregnancy? |
-Fetal radiation dose is considered low for both lung scintigraphy and CTPA -However maternal radiation dose is much higher for CTPA -Carcinogenesis induced by low lvl radiation is considered the major risk factor for both mother + fetus -Lung and breast cancer are two malignancies that account for greatest risk of radiation induced cancer mortality -Imaging modality of choice still debated -Higher maternal dose, including breast dose with CTPA -Whether or not fetal dose is different is unclear -Can often do a reduced dose perfusion only V/Q scan in pregnant pts -Unilateral leg swelling --> get US (least problematic) |
|
|
Findings indicating a benign pulmonary nodule on CXR |
-Benign pattern of calcification -Not all benign nodules (including granulomas) are calcified -Nodule stable at least 2 years is consistent with benign etiology (compare with prior CXRs) |
|
|
4 benign patterns of calcification |
Central Diffuse solid Laminated Popcornlike |
|
|
What is useful for nodules after CXR? |
If may be unclear whether or not a nodule is calcified on CXR - chest CT is useful in further evaluation If chest CT shows a benign pattern of calcification no additional follow-up is needed |
|
Pattern of calcification |
Central - benign |
|
|
If nodule on CXR is indeterminate or suspicious for cancer, then ____ is the next imaging test |
non-contrast chest CT |
|
|
Factors to consider when evaluating a nodule: |
-Patient's age (younger = less likely cancer) -Smoking history --> 80% chance of lung cancer -Radiologic appearance of nodule: 1) Size: <8 mm <1% chance of cancer 2) Shape 3) Edge characteristics 4) Calcification |
|

Tumor type? |
Hamartoma - low attenuation of fat visible |
|
|
Lung caner is more likely if the nodule has a _____ or _____ |
lobulated contour or irregular spiculated margins |
|
|
FDG PET/CT |
-Typically for nodules >1 cm -18F-FDG accumulation occurs in many malignant nodules -Infectious nodules, including granulomas, may also be PET + (false positive) -Some neoplasma may be PET -, particularly indolent adenocarcinomas and carcinoid tumors (false negatives) |
|
|
Lung cancer vs granulomatous infection on radiography |
Can have similar radiographic appearance + similar CT appearance and both can demonstrate increased FDG uptake on PET Biopsy often required to confirm pathology (benign or malignancy) |
|
Pathology? |
Cavitated pulmonary nodule |
|
|
What is a convern with cavitary nodules? |
Tuberculosis - especially if they are located in the upper lobes or superior segment of the lower lobes Multiple small adjacent nodules suggest infection |
|
Pathology? |
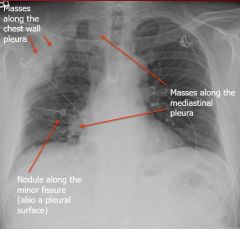
malignant mesothelioma |
|

Pathology? |
Sarcoid - see bilateral hilar adenopathy |
|
|
CXR findings in sarcoidosis |
-Textbook: bilateral hilar adenopathy -CXR can be nonspecific in these pts -Can have multiple small pulmonary nodules which are predominantly in the upper half of the lungs |
|
|
CT findings in sarcoid |
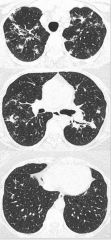
Upper zone - multiple small pulmonary nodules; many other variations (no pulmonary findings, alveolar, focal) |
|
Findings? |
Sarcoid |
|
|
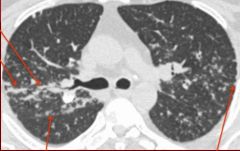
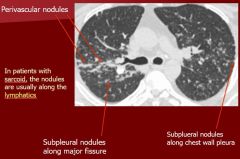
In pts with sarcoid, nodules are usually found along the ___ |
lymphatics |
|
Findings? |
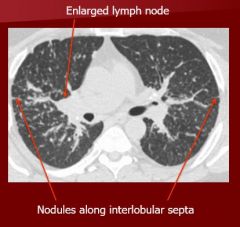
Sarcoid |
|
|
Hypersensitivity pneumonitis CXR findings (slide 102) |
Chest radiograph demonstrates patchy airspace disease and multiple ill-defined lung nodules |
|
|
Hypersensitivity pneumonitis CT findings (slide 103) |
-Ill-defined ground glass nodules -Upper zone predominance -No other findings that indicate pulmonary edema (diffentiates) |
|
|
Patients with UIP usually demonstrate greater lung involvement in the ____ |
lower zones |
|
|
Typical imaging finding for UIP? |
Areas of normal lung interspersed with areas of diseased lung Honeycombing in late stages |
|
Findings? |
Usual interstitial pneumonia |
|
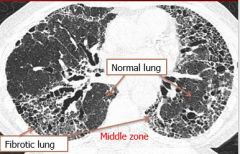
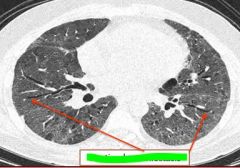
Findings? |
Intersitial fibrosis - UIP pattern (fibrosis more prominent in lower zones) |
|

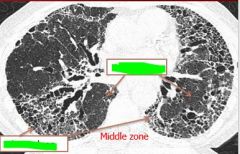
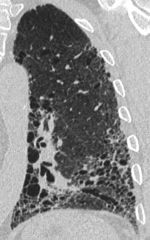
Findings? Where is this typically found in the lung? |
The lung involvement in UIP typically has a peripheral distribution Can see honeycombing |
|
|
Pts with diffuse alveolar damage usually have _____ |
diffuse lung involvement - ARDS most common cause, also potentially AIP |
|
Findings? |
Diffuse alveolar damage |
|
|
Organizing pneumonia CXR findings |

Multiple patchy airspace opacities Not infectious - does not go away with abx |
|
|
Differentiate ground glass vs consolidation |
-Ground glass opacity is hazy increased opacity of the lung with preservation of bronchial and vascular margins -Consolidation appears as homogenous increase in pulmonary parenchymal attenuation that obscures the margins of vessels and airway walls |
|

Pathology? Indicative of...? |
Intrapulmonary Cysts - ARDS |
|
Pathology? Indicated of...? |
Traction bronchiectasis - see dilated vessels out in the periphery - indicative of ARDS |
|

Pathology? |

Cavitated pulmonary nodule |