![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
69 Cards in this Set
- Front
- Back
|
Conduction system through the heart |
electrical impulse begins at SA node--> travels across atria = atrial contraction--> impulse arrives at AV node--> travels through Bundle of HIs--> conducted through ventricle--> depolarization (contraction) of ventricle |
|
|
EKG represents depolarization & repolarization depolarization= ______________ repolartization=______________ |
depolarization= contraction REpolarization= RElaxation |
|
|
____ wave = atrial depolarization (contraction)
|
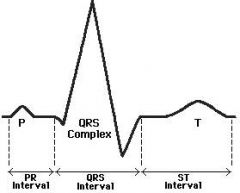
P wave |
|
|
____ (wave) complex = ventricular depolarization (contraction) |
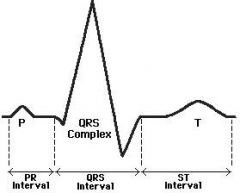
QRS complex (wave) |
|
|
___ wave = ventricular repolarization (relaxation) |
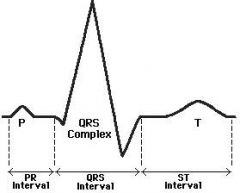
T wave |
|
|
_____ interval = time between atrial & ventricle firing (initial stimulation) |
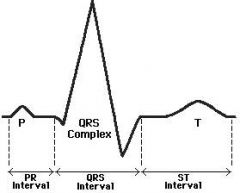
PR interval |
|
|
____ interval = time it takes ventricle to completely depolarize |
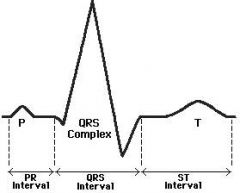
QRS interval |
|
|
____ interval = time it takes ventricle to repolarize |
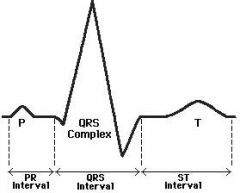
ST interval |
|
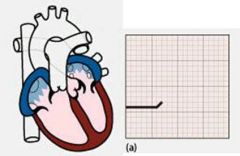
When 1/2 the atria has depolarized what occurs? |
top of P wave= electrical potential is at max= atrial firing |
|
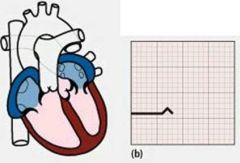
When the atria is completely depolarized, what occurs? |
bottom of P wave= electrical potential = 0 |
|
When 1/2 the ventricle depolarizes, what is occuring? |
top of R wave= ventricle firing |
|
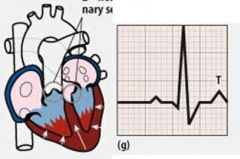
After the ventricle has depolarized & reached 0, what occurs when the T wave becomes (+)? |
T wave = repolarization of ventricle |
|
|
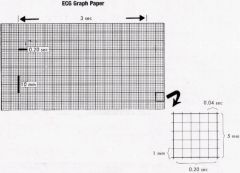
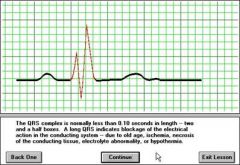
Know how to read ECG on graph |
|
|

After the P wave, the first downward deflection is the _____wave & the first upward deflection is the R wave. If the first deflection is upward, there is no _____ wave |
Q wave
Q wave
(there may NOT be a Q wave if the first deflection after the P wave is upward!) |
|

After the R wave, the first downward deflection is the ____ wave. (If the downward deflection is BEFORE the R wave, it is the Q wave**) |
S wave
(always comes after R wave, regardless if there is a Q wave present) |
|
If there are 2 downward deflections following a P & R wave, what are they called? (NO g wave!) |
S & S prime wave (image other side)
(may also be R & R prime if there are 2 upward deflections in a row after P wave, image)) |
|
|
If there is one single downward deflection after the P wave (NO R wave), what is it called? |
QS wave |
|

At the peak of the P wave, the atria contracts & the first _______ is seen At the peak of the QRS wave, the ventricle contracts & the second, larger ______ is seen |
small pressure spike is seen
larger pressure spike is seen |
|

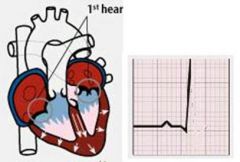
The rise of the large pressure curve, corresponding to ventricular contraction, occurs at the same time as the ______ |
1st heart sound = S1 = ventricle contracts
|
|

The fall of the large pressure curve occurs at the same times as the __________ |
2nd heart sound = S2 = aortic & pulmonic valve closing |
|
|
Two types of leads |

chest leads (6) limb leads (4)
(usually only use 3, both arms & 1 foot for limb leads) |
|
|
Different leads provide different views of the heart on EKG. Always going from ____--> _____
|
always from (-)--> (+) |
|
|
Limb leads view the heart from the _____ plane |
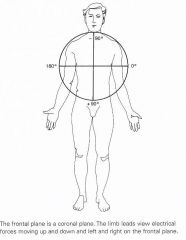
coronal/frontal plane |
|
|
Limb leads I, II, III |
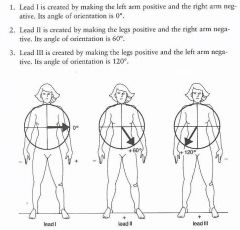
I: arm leads only = 0 II: legs + & R arm - = +60 III: legs + & L arm - = +120
(arm lead travels from shoulder) |
|
|
Limb leads AVL, AVR, AVF |
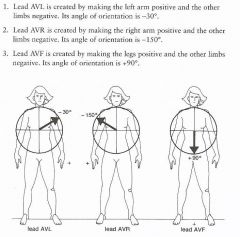
AVL: L arm +, rest - = -30 AVR: R arm +, rest - = -150 AVF: legs +, arms - = +90 |
|
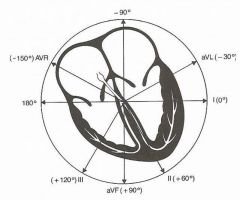
arrows point to what? |
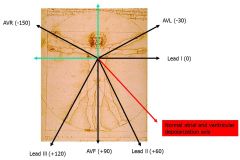
where you are looking at heart from |
|
|
If atrial or ventricular depolarization is traveling towards a lead at less than 90 degrees, there will be a positive deflection & R ____ S |
less than 90 R > S
|
|
|
If atrial or ventricular depolarization is traveling at a 90 degree angle to a lead, the deflections will be isoelectric (+ deflection = - deflection) & R _____ S |
equal to 90 R = S
|
|
|
It atrial or ventricular depolarization is traveling at an angle greater than 90 from the lead, the deflection will be negative & R _____S |
greater than 90 R < S
*the only limb lead w a negative deflection should be AVR |
|
|
Where are the 6 chest leads placed? Chest leads view the heart from what orientation? |
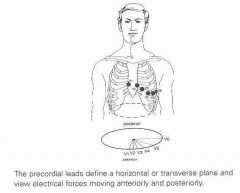
horizontal/transverse plane
V1 & 2- R & L sternal border V3- btwn V2 & 4 V4- mid clavicular (below nipple) V5- btwn 4 & 6 V6- mid axillary |
|
|
Where do the chest leads view the heart from? |

|
|
|
If the SA node is dysfunctional, what other pacemaker tissues can set the heart rate? at what rates do they fire? |
atria- 75 bpm (similar to SA, normal HR) AV node- 60 bpm ventricle- 40 bpm
(go in order--> if atria doesnt work AV will set, etc) |
|
|
How can you determine the rate of a regular rhythm (quick method)?
(should be btwn 60-100 bpm) |
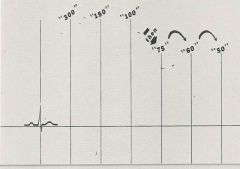
(P wave in front of each QRS = regular rhythm) (equidistant R peaks = regular rate)
Count the # of large boxes (ms) btwn each R 1= 300 2= 150 3= 100 (then 75, 60, 50)
|
|
|
How can you determine the rate of an irregular rhythm? |
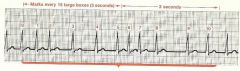
(no P wave = Irregular rhythm)
count out 30 large boxes (6 seconds). take the # of R waves in 30 boxes * 10 = R waves /60 sec (bpm) |
|
|
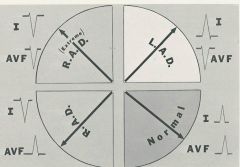
A normal QRS axis is btwn ____ & _____ |
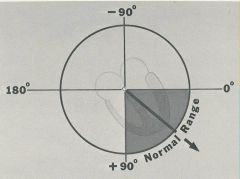
0 & + 90 |
|
|
Any QRS btwn 0 & -90 is considered ________
What causes this? |
left axis deviation (LAD)
severe pulmonary htn w/ RVH or LV infarct |
|
|
Any QRS btwn +90 & -90 is considered _______
What causes this? |
right axis deviation (RAD)
abdominal obesity, LVH, RV infarct |
|
|
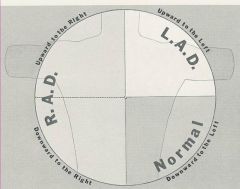
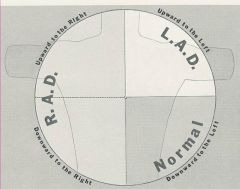
How can you determine the QRS orientation using leads I & AVF? |
|
|
|
____ block miss a complete cycle (a P & QRS are missing), but the rate is consistent. |
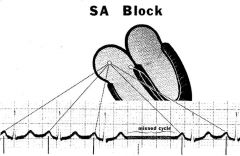
caused by a lack of impulse from the SA node |
|
|
______ block, creates a delay after P way (before ventricles are stimulates), prolonging the PR interval > 0.2 sec or 1 large block (distance btwn beginning of P & beginning of R)
(PR interval also cannot be < 0.08/2 small boxes) |
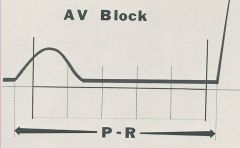
first degree AV block |
|
|
______ block occurs when it takes 2 or more P waves (atrial impulses) to stimulate a QRS (ventricle impulse)
named 2:1 = 2 P waves per 1 QRS, may be 3:1
(QRS morphology should be normal) |
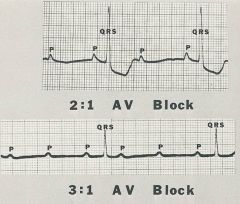
second degree AV block |
|
|
__________ is a 2nd degree block that occurs when the PR interval becomes progressively longer until a QRS is dropped, then shorter again |
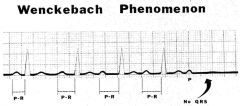
(Mobitz I block) |
|
|
______ is a 2nd degree block that occurs when the PR interval remains the same, but the QRS is still dropped
*UNSTABLE rhythm |
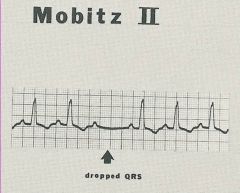
Mobitz II |
|
|
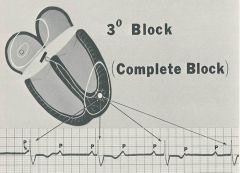
________ block occurs when no atrial impulses stimulate the AV node (atria & ventricles are completely dissociated), ventricles paced independently
*UNSTABLE rhythm |
|
|
|
______ block results in an R & R' wave due to split ventricular firing (should fire simulataneously), the QRS interval is > 0.12 or 3 small boxes
(if QRS is normal this is an incomplete block) (these may be rate dependent) |
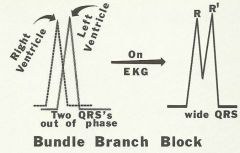
bundle branch block (whichever side blocked will have delayed firing) |
|
|
(left/right) bundle branch block results in R & R' on V1 & V2 (these look at ant chest- RV) The left ventricle fires first |
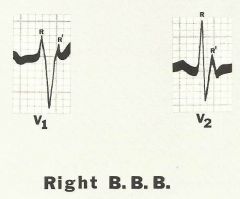
Right bundle branch block |
|
|
(left/right) bundle branch block results in R & R' on V5 & V6 (these look at lateral chest, LV) Right ventricle fires first
*THIS IS AN EMERGENCY--> MI (if new) |
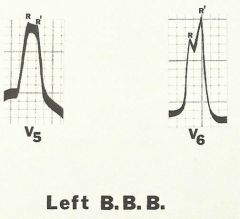
Left bundle branch block |
|
|
Which blocks are stable? |
1st degree AV block 2nd degree AV block Wenckebach (mobitz I) Chronic Bundle branch blocks |
|
|
which blocks are unstable (emergency)? |
Mobitz II New bundle branch blocks 3rd degree blocks |
|
|
Which leads should you look at for atrial hypertrophy? |

II & V1 P waves* |
|
|
what leads do you look at for P mitrale? |
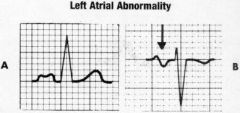
II- broad humped P V2- biphasic wide P w/ downward deflection |
|
|
what leads do you look at for P pulmonale? |
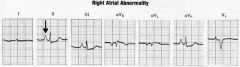
Peaked P in II & V1 |
|
|
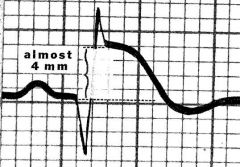
ECG findings in LVH |
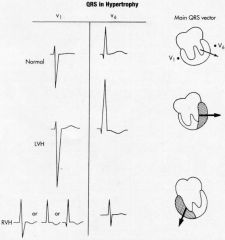
* QRS complex V1- deepened S wave V6- taller R wave
S wave (V1) + R wave in (V6) = >35mm
R wave (aVL) > 11mm = strain |
|
|
ECG findings in RVH |
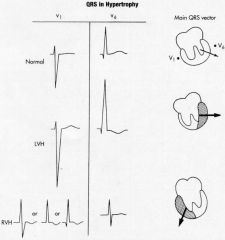
*QRS V1- tall R wave V6- biphasic QRS complex |
|
|
ECG findings in Left Anterior Fascicular Block (LAFB) |

-left axis deviation (NO QRS widening, hypertrophy, or strain) |
|
|
Ischemia (lack of blood supply) is represented by _________________ or _________________ |
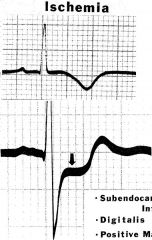
symmetrically inverted T waves (top) or ST segment depression w/ normal T wave (bottom) |
|
|
Ongoing injury (prolonged ischemia) is represented by ______________ of 1 mm or more
-T waves may be normal, inverted, or peaked
*EMERGENCY*** treat for MI |
ST elevation >1 mm |
|
|
Transmural infarction (irreversible injury) produces significant _______________ |
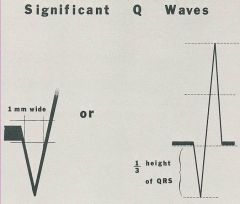
Q waves ^ either 1 box wide OR 1/3 total height of R |
|
|
Ischemia/Injury/infarct can be localized based on the leads that show findings. ST elevation & peaked T waves in leads V1, V2, V3, V4, V5, shows ongoing injury (evolving infarct) where? |
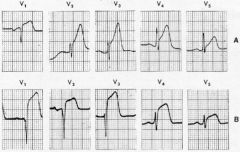
anterolateral infarct is occuring |
|
|
ST elevation & peaked T waves in leads II, III, aVF shows an evolving infarct where?
*firemans hat appearance |
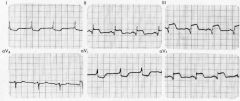
inferior infarct |
|
|
ST elevation & peaked T waves in leads I, aVL, V5, & V6 shows infarct where? |
lateral infarct |
|
|
ST elevation & peaked T waves in leads V3 & V4 shows infarct where? |
anterior infarct |
|
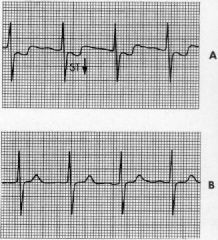
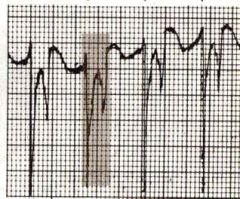
What does the ST depression in A signify?
B is after treatment w/ nitroglycerin |
ST depression signifiies ischemia of subendocardial injury |
|
|
What does Hyper K+ show on ECG? |
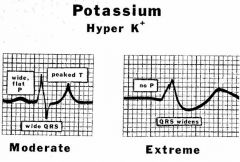
*wide QRS + no P is very DANGEROUS = extreme hyperkalemia--> infarct |
|
|
What does Hypo K+ show on ECG? |
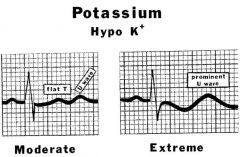
U wave
(not as serious as hyper) |
|
|
What is more dangerous, hypercalcemia or hypocalcemia? Why? |
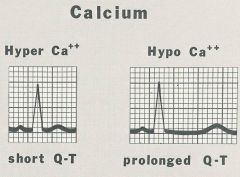
HYPOcalcemia- prolongs repolarization--> can cause V tach or V fib
(hyper shortens QRS) |
|
|
Pt comes in w/ chest pain ECG: diffuse flat ST elevations across precordium (all) reciprical ST depression in aVR only low amplitude R waves (every lead)
what pathology? |
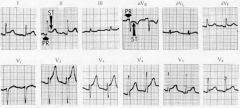
Pericarditis |
|
|
What effect does digitalis have on ECG? |
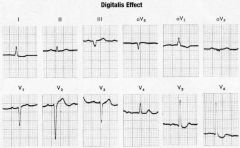
(if toxic will show AV block) |
|
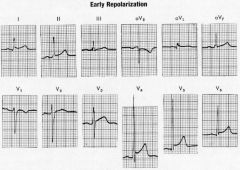
what patients is this common in? |
athletes |