Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
129 Cards in this Set
- Front
- Back

|
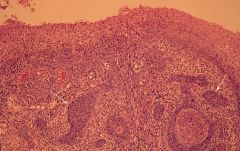
Vulva – Condyloma acuminatum
The white “cauliflower” papillomatous lesions (arrow) are condyloma acuminata. |
|

|
Vulva – Condyloma acuminatum
The white “cauliflower” papillomatous lesions (arrow) are condyloma acuminata. |
|
|
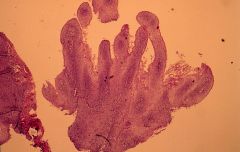
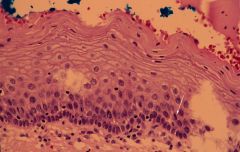
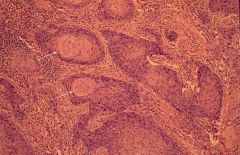
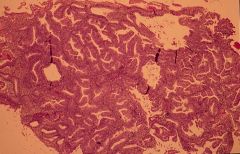
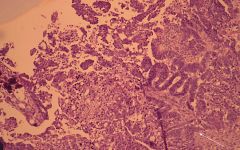
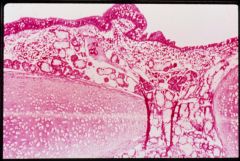
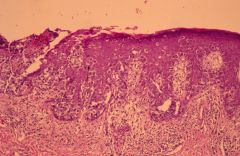
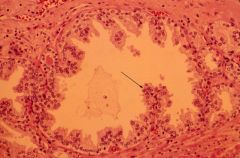
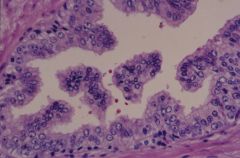
Condyloma acuminatum
Papillomatous lesion represented by finger like projections lined by squamous epithelium with koilocytosis (koilocytosis can not be appreciated in this image, see next image). |
|
|
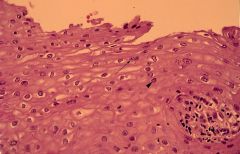
Condyloma acuminatum
Papillomatous lesion represented by finger like projections lined by squamous epithelium with koilocytosis (koilocytosis can not be appreciated in this image, see next image). |
|

|
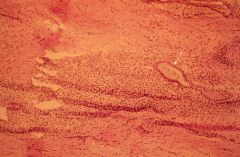
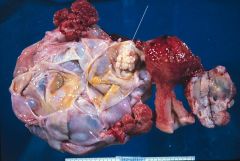
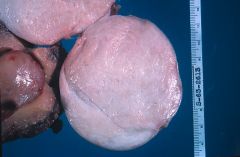
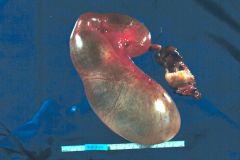
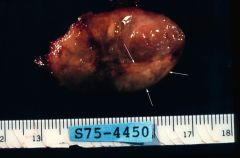
Vulva-Squamous cell carcinoma
Exophytic white mass having gross features similar to a condyloma acuminatum in this case. This case would require microscopic evaluation to make the diagnosis. |
|

|
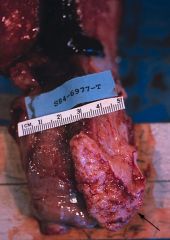
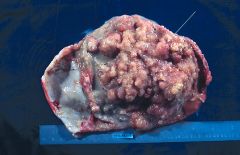
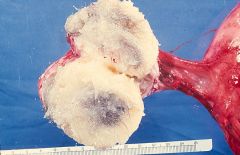
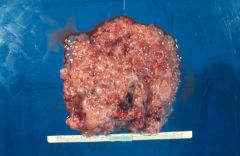
Vulva-Squamous cell carcinoma
An exophytic mass has been sectioned. The tan fleshy tissue represents invasive carcinoma. |
|
|
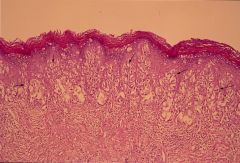
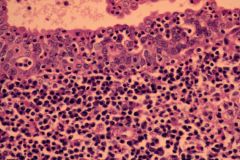
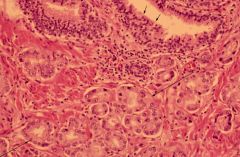
Paget’s disease of vulva (Extramammary Paget’s Disease)
The epidermis contains nests of larger epithelial cells with clear cytoplasm and pleomorphic hyperchromatic nuclei (arrows). The clear cells contain intracytoplasmic mucin. |
|

|
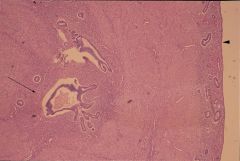
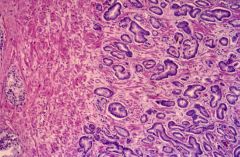
Cervix – Squamous cell carcinoma
Large exophytic, tan-brown, ulcerated mass grossly representing invasive squamous cell carcinoma. |
|
|
Cervix – Squamous cell carcinoma
Cervix has been opened longitudinally. It contains a tan-fleshy mass with a tumor epicenter at the squamocolumnar junction. Tumor extends to ectocervix and into the endocervical canal (arrow). |
|

|
Cervix – Squamous cell carcinoma
Slightly exophytic, ulcerated, tan-brown mass of ectocervix (arrow). Grossly represents a cervical squamous cell carcinoma. |
|
|
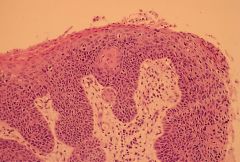
Cervix – Mild dysplasia (low grade dysplasia)
This patient had a pap smear interpreted as mild dysplasia and this represents a cervical biopsy. The lower one-third thickness of the squamous epithelium exhibits increased cellularity with nuclear hyperchromasia and occasional mitosis (arrow). |
|
|
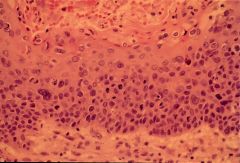
Cervix – High grade dysplasia
The lower one-half thickness of the epithelium exhibits increased cellularity, abnormal maturation of squamous cells, nuclear pleomorphism, hyperchromasia, and mitotic activity. This is an example of high grade dysplasia which incorporates moderate dysplasia and severe dysplasia. Koilocytotic features representing HPV effect are present. |
|
|
Cervix – High grade dysplasia
The lower one-half and lower two-thirds (focally) thickness of the epithelium exhibits increased cellularity, abnormal maturation of squamous cells, nuclear pleomorphism and hyperchromasia, and mitotic activity. This is an example of high grade dysplasia which incorporates moderate dysplasia, and severe dysplasia, koilocytotic features representing HPV effect are present. |
|
|
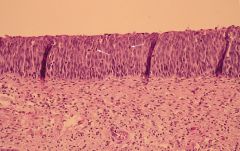
Cervix - CIS
Full thickness abnormal maturation is present. Cellularity is increased with nuclear hyperchromasia and pleomorphism. Mitoses extend toward the surface (arrow). |
|
|
Cervix – Microinvasive squamous cell carcinoma
Nests of invasive squamous cells are invading superficially (less than 5 mm) into the submucosa (arrows). Horizontal dimension must be less than 7mm. |
|
|
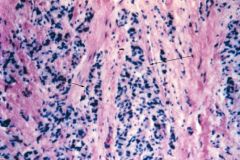
Squamous cell carcinoma
Nests of malignant squamous cells are invading into an inflamed reactive fibrous stroma. The nests contain squamous cells with cytologically malignant nuclei (hyperchromatic and pleomorphic). Some cells contain eosinophilic cytoplasm and there is keratin pearl formation (arrows). |
|

|
Squamous cell carcinoma
Nests of malignant squamous cells are infiltrating reactive fibrous stroma. |
|
|
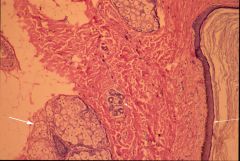
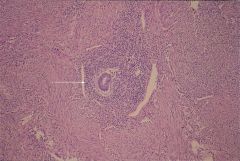
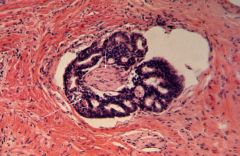
Peritoneum: Endometriosis
Nests of endometrial stroma and glands (arrow) are present within the fibrous stroma. |
|

|
Uterus – Adenomyosis (gross)
Myometrium contains a tan fleshy tissue nodule representing adenomyosis (arrow). The remainder of the myometrium is trabeculated (irregular) appearing. Slit-like spaces may be seen in a trabeculated myometrium in adenomyosis. |
|

|
Uterus - Adenomyosis
Myometrium has a trabeculated appearance with slit-like spaces which are hemorrhagic appearing (arrows). |
|
|
Uterus – Adenomyosis
An arrowhead points to the endometrial cavity surface. The long arrow points to the nests of endometrial glands and stroma within the myometrium. |
|

|
Uterus - Adenomyoma
Uterus contains a nodular, trabeculated mass with slit-like spaces (arrowhead). There is a larger hemorrhagic area (large arrow) also present. This and the slit-like spaces represent endometrial stroma and glands. The remainder of the nodule is represented by proliferating smooth muscle. |
|

|
Uterus - Leiomyomata
Cut section of gray-white whorled intra-mural masses which would be firm to rubbery on palpation. |
|

|
Uterus - Leiomyomata
Multiple sub-serosal, irregular shaped masses representing leiomyomas (fibroids). |
|

|
Uterus - Leiomyoma
A submucosal nodular mass (arrow) fills the endometrial cavity representing a leiomyoma. |
|

|
Uterus - Leiomyoma
Leiomyomas sometimes undergo degenerative changes including infarction. This is represented grossly as softening with brown or red discoloration known as brown degeneration (arrow head). The long arrow represents an undected intrauterine pregancy. |
|

|
Uterus – Leiomyoma (micro)
Myometrium containing an ill-defined mass of benign smooth muscle cells which intertwine with one another (arrows around leiomyoma – fibroid). |
|
|
Uterus – Leiomyoma (micro)
The cellularity on the left is higher than on the right. Smooth muscle cells contain “cigar” shaped nuclei (arrow) which are cytologically benign and exhibit no mitotic activity. |
|
|
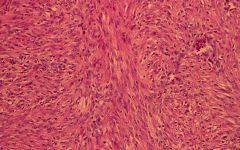
Uterus - Leiomyoma (micro)
High power view of smooth muscle cells forming fascicles and bundles which intertwine with each other. Nuclei have benign cytologic features without atypia or mitotic activity. |
|

|
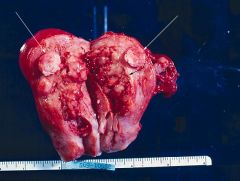
Uterus - Leiomyosarcoma
Uterus and cervix have been opened. The uterus contains a gray-white fleshy mass (arrow) representing a leiomyosarcoma. |
|
|
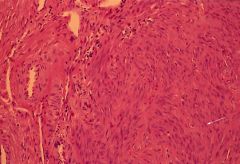
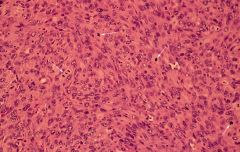
Uterus – Leiomyosarcoma (micro)
Spindle shaped smooth muscle cells exhibit slightly pleomorphic nuclei which are hyperchromatic. There is abundant mitotic activity present (arrows). Mitotic activity is the most important feature used to distinguish a leiomyoma from a leiomyosarcoma. |
|

|
Uterus – Endometrial adenocarcinoma
(Adnexa – short arrow, endocervical canal – long arrow, tumor – bold arrow). The endometrial canal contains a fungating, cauliflower, tan, fleshy mass representing endometrial adenocarcinoma. |
|
|
Uterus – Endometrial adenocarcinoma
A tan-red fleshy mass (short arrow), fills the endometrial cavity representing endometrial adenocarcinoma. Leiomyomas are also present (long arrows). |
|

|
Uterus – Endometrial adenocarcinoma
(Ovary – short arrow, cervix – long arrow, tumor – bold long arrow, tumor invading myometrium – bold short arrow). The endometrial cavity is dilated and contains a large tan-brown to gray mass which can be seen focally invading myometrium (bold short arrow). |
|

|
Uterus – Endometrial adenocarcinoma
(Cervix – short arrow, endometrial adenocarcinoma – long arrow). This is a longitudinal section of cervix and uterus. The endometrium has been replaced with lush, white fleshy tissue (long arrow) representing endometrial adenocarcinoma. |
|
|
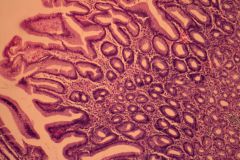
Endometrium – Atypical complex (adenomatous) hyperplasia
The gland to stroma ratio is increased and the glands exhibit complex architecture represented by micro-villous and papillary projections into the lumen of the glands. This is from a 65-year-old obese, diabetic women with post-menopausal bleeding. |
|

|
Uterus-cervix-Sarcoma botryoides (rhabdomyosarcoma)
Endocervix and uterus contain an irregular mass containing “grape-like” appearance (top of specimen). |
|

|
Uterus – cervix – Sarcoma botryoides (rhabdomyosarcoma)
High power view revealing grape-like architecture (arrow) of the tumor. |
|

|
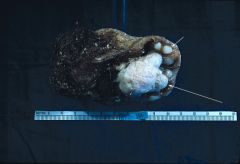
Ovary – Serous cystic tumor (cystadenoma)
A large gray-white and gray-blue mass has replaced the ovary on the left (arrows). It would be soft to palpation and filled with yellow-clear non-viscous fluid. Microscopic studies would be necessary to differentiate a benign form from “undetermined malignant potential” type from a malignant form. |
|
|
Ovary – Serous cystic tumor (cystadenoma)
The ovarian tumor on the left has been opened. It was filled with yellow-clear non-viscous fluid. The majority of the inner surface of the cyst is smooth (small arrows). Note the more solid papillomatous area (large arrow). This is the area which needs to be evaluated histologically to differentiate a benign, malignant and borderline (undetermined malignant potential) form from each other. |
|
|
Ovary – Serous cystic tumor (cystadenocarcinoma)
This serous tumor exhibits a more extensive thickened papillae inner surface (arrows). Histologically, it proved to be adenocarcinoma. |
|
|
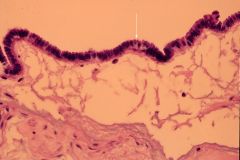
Ovary – Serous cystadenoma (micro)
The cyst is lined by a single layer of serous cells columnar, non-mucin producing cells with cilia (arrow). |
|
|
Ovary – Serous cystadenocarcinoma (micro)
The serous type epithelium is more complex architecturally and invades into the stroma of the ovary (arrow). Definitive ovarian stromal invasion distinguishes a borderline tumor from an adenocarcinoma. |
|

|
Ovary – Mucinous cystadenocarcinoma
This is a cut section of an ovarian cystic neoplasm. The cysts contain tan to gray-white gelatinous mucoid material. Histologically, the tumor was malignant. |
|
|
Ovary – Mucinous cystic neoplasm (micro)
Mucinous neoplasms of the ovary are lined by cells which exhibit mucinous differentiation. These cystic structures are lined by columnar cells, which contain clear cytoplasm representing mucin. In benign mucinous tumors, the cysts are lined by a single layer of epithelial cells, in a borderline tumor (undetermined malignant potential), they are lined by multiple layers of epithelium with complex architecture (papillae, cribriform pattern, microvillous structures). In a carcinoma there is ovarian stromal invasion and cytologically the epithelial cells exhibit malignant features. |
|
|
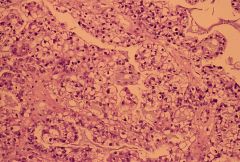
Ovary – Clear cell carcinoma
This is a high grade adenocarcinoma of the ovary (it may also occur in the endometrium, cervix and vagina). The tumor cells are large due to abundant optically clear cytoplasm. Nuclei exhibit hyperchromasia and pleomorphism, and are usually eccentric in location. |
|

|
Ovary – Krukenberg tumors
Bilateral ovarian tumors (arrows) represented by tan, fleshy cerebriform masses which histologically are represented by signet ring carcinoma. These represent ovarian metastases from a ****gastric primary adenocarcinoma****. |
|
|
Ovary – Krukenberg tumor (micro)
Sheets of signet rings are present (arrows). Signet rings are represented by large polyhedral cells with abundant mucinous to clear cytoplasm containing a peripherally displaced crescent-shaped, hyperchromatic nucleus. The cells contain intracytoplasmic mucin. |
|
|
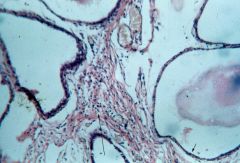
Ovary - Fibroma
A large chalky-white fibrous mass. This fibroma would be firm to rubbery on palpation. |
|

|
Ovary – Fibroma
Endometrium – Endometrial polyp The adnexal mass on the right (long arrows) represent a fibroma. It is a circumscribed white trabeculated mass reminiscent of a leiomyoma. The short arrow is pointing to an endometrial polyp which is a tan-velvety polypoid structure filling the endometrial cavity. |
|
|
Ovary – Cystic teratoma (mature)
This sectioned cystic ovarian mass is filled with whitish greasy gruminous material containing hairs. Prior to sectioning, it would be doughy feeling when palpated. |
|
|
Ovary – Cystic teratoma (mature)
This is a cystic mass containing numerous hairs and teeth (small arrow). The large arrow points to a nodule in the mass called Rokitansky’s nodule which contains all of the teratomatous elements. |
|
|
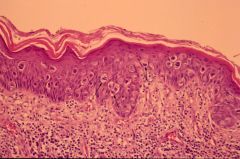
Ovary – Mature cystic teratoma (dermoid cyst) - micro
This section of a cystic teratoma contains skin represented by epidermis (long arrow), sweat glands (short arrow), and sebaceous glands (bold arrow). There is also adipose tissue present. All elements are mature. |
|
|
Ovary – Mature cystic teratoma
This section contains respiratory epithelium, mucinous and serous acini, and cartilage. All elements have mature features (non-fetal appearing tissue seen normally in adults). |
|
|
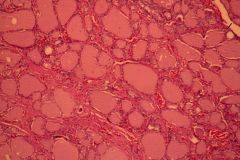
Ovary – Mature cystic teratoma
This teratoma contained thyroid tissue. Tumors composed only of thyroid tissue are also known as struma ovarii. |
|
|
Ovary – Mature cystic teratoma
This portion of Rokitansky’s nodule contains gastric type mucosa. |
|

|
Ovary – Endometriotic cyst (chocolate cyst)
The ovary on your left has a large cystic mass filled with long standing blood clot which as the appearance of melted chocolate (arrow). This represents an area of cycling endometriosis, which repeatedly bleeds creating a “chocolate cyst”. |
|

|
Ovary – Endometriotic cyst
This cyst has a green to brown colored appearance of the inner wall. This represents old hemorrhage and hemosiderin (iron) deposits in the wall of the cyst. |
|

|
Ovary – Hemorrhagic corpus luteum cyst
Normally a corpus luteum develops after ovulation. Sometimes it can become large and cystic to the degree it may presently clinically as an ovarian mass. The center of the cyst is represented by blood clot (short arrow). The outer wall of the cyst in some areas (long arrow) contains a thin yellow ribbon of tissue which is sometimes convoluted appearing representing luteinized granulosa cells and thecal cells. |
|

|
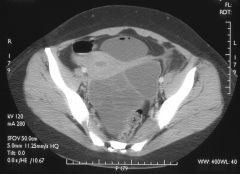
Ovarian Dermoid Cyst - CT image at level of mid pelvis demonstrates a rounded mass on the right. There is a fat-fluid level within this mass with a mixed density structure floating at the fat-fluid interface (“dermoid plug” or Rokitansky nodule). The wall of this mass is partially calcified.
|
|

|
Cystadenoma - Transvaginal ultrasound image demonstrates a multiseptated cystic mass within the pelvis.
|
|
|
Cystadenoma - CT image at the level of the lower pelvis demonstrates a multiseptated cystic mass posterior and to the left of the uterus displacing the uterus anteriorly and to the right.
|
|

|
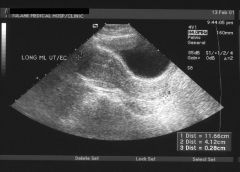
Simple Ovarian Cyst - Transabdominal ultrasound image of the uterus and ovaries demonstrating a cyst of the right ovary..
|
|

|
Simple Ovarian Cyst - Transabdominal ultrasound of the right ovary demonstrates the ovarian mass to be well circumscribed and anechoic.
|
|

|
Ovary – Tubo-ovarian abscess
This is a large adnexal cystic mass filled white-creamy purulent material (pus) forming an abscess. |
|
|
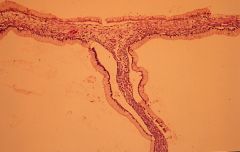
Fallopian tube - Hydrosalpinx
Sausage-shaped dilation of fallopian tube seen in chronic salpingitis. This structure has gross features of a benign peri-tubal cyst, however, it communicated with the lumen of the fallopian tube in a patient with chronic salpingitis. |
|
|
Fallopian tube – chronic salpingitis
Numerous plasma cells (arrow) and lymphocytes are present within plicae of the fallopian tube. Plasma cells must be present before the diagnosis of chronic salpingitis can be made. |
|

|
Fallopian tube: Ectopic pregnancy
This fallopian tube exhibits a red or hyperemic sausage shaped region of dilation representing a non-ruptured ectopic pregnancy. |
|

|
Fallopian tube: Ectopic pregnancy
The fallopian tube has been opened. It is cystic and contains an inner shaggy-spongy, red to brown wall representing placental tissue surrounding a small fetus with umbilical cord. Finding an intact fetus in an ectopic pregnancy is unusual. |
|

|
Fallopian tube: Ruptured ectopic pregnancy
Note the rupture site of this ectopic pregnancy. Rupture is the most serious complication of an ectopic pregnancy, which can result in life-threatening hemorrhage. |
|
|
Fallopian tube - Endometriosis
The wall of the fallopian tube containing nest of endometrial stroma and glands (arrow). |
|

|
Tubo-ovarian abcess - Irregularly shaped multilocular complex mass abutting uterus on left.
|
|

|
Tubo-ovarian abcess - Multilocular complex mass.
|
|

|
Tubo-ovarian abcess - Multilocular cystic mass abutting uterus on left with air-fluid levels within the mass.
|
|
|
Hydatidiform mole
This is tissue expelled from a women representing a hydatidiform mole. It is represented by a mass having the appearance of a “bunch of grapes”. |
|
|
Transabdominal US demonstrating absence of intrauterine pregnancy.
|
|

|
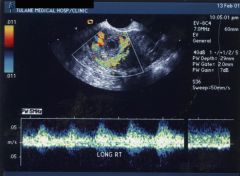
Heterogeneous echogenic mass in right adnexal region.
|
|
|
Color Doppler image demonstrating high velocity flow around the adnexal mass reflecting the increased peritrophoblastic blood flow at the implantation site.
|
|

|
(Choriocarcinoma) - Transabdominal ultrasound demonstrates a very subtle area of decreased echogenicity in the fundus of uterus.
|
|

|
(Choriocarcinoma) - Color Doppler evaluation of uterus demonstrates a focal area of markedly increased blood flow reflecting increased peritrophoblastic flow in this patient with myometrial invasion by the choriocarcinoma.
|
|

|
(Choriocarcinoma) - Hypodense mass is present in the fundus of the uterus.
|
|

|
Lung Metastases from Choriocarcinoma - Multiple rounded masses are present within both lungs consistent with hematogenous spread of the choriocarcinoma.
|
|

|
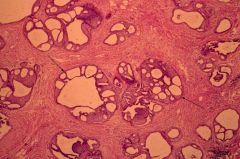
Breast – Fibrocystic disease
This breast tissue contains increased white-gray fibrous tissue (short arrow) and multiple small cysts, some of which have blue-gray color representing “blue-domed cyst” (long arrow). |
|
|
Breast – Fibrocystic disease
Ducts are cystically ectatic or dilated (small arrow) and they are separated by fibrous stroma (long arrow). |
|

|
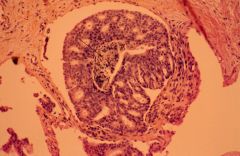
Breast – Intraductal papilloma
This breast biopsy contains a dilated duct (small arrow) which is filled with a light brown-gray papillomatous mass (long arrow). These usually presents clinically with a bloody nipple discharge. |
|

|
Breast - Fibroadenoma
This is a spherical nodule which is circumscribed appearing. They are tan to gray in color and usually rubbery to soft when palpated. |
|

|
Breast - Fibroadenoma
Round, circumscribed appearing nodular mass containing slit-like spaces which represent ductular structures in the tumor. The left side represents the cut surface, the right side represents the outer surface which appears circumscribed. |
|

|
Breast – Infiltrating carcinoma
The tumor is represented by a stellate white hard mass (arrow). Sometimes pinpoint areas of yellow color representing necrosis of tumor (comedonecrosis) can be seen. |
|

|
Breast – Infiltrating carcinoma
The tumor is represented by a light-gray to white irregular firm mass (small arrow). There are pinpoint areas of yellow discoloration representing comedonecrosis (long arrow). |
|

|
Breast – Infiltrating carcinoma
This section contains skin and nipple. Deep to the nipple is a gray to light tan mass (long arrows) with pinpoint yellow colored areas (short arrow). |
|

|
Breast – Paget’s disease of nipple and infiltrating carcinoma
The nipple on the left is centrally ulcerated. The breast tissue on the right contains an irregular gray-white mass (arrows) representing infiltrating carcinoma. |
|
|
Breast – Paget’s disease of nipple
The epidermis contains numerous large pale cells containing cytologically malignant nuclei (arrows). The pale cytoplasm represents intracytoplasmic mucin. |
|
|
Breast – Paget’s disease of nipple
The epidermis contains numerous large pale cells containing cytologically malignant nuclei (arrow). The pale cytoplasm represents intracytoplasmic mucin. |
|
|
Breast – Ductal carcinoma in situ (CIS)
Dilated ducts (arrows) contain ductal cellular proliferations creating a cribriform pattern. The cribriform spaces or clear spaces have the appearance of being made with a cookie-puncher, creating round symmetrical clear spaces like cookies were removed. No invasive tumor is present. |
|
|
Breast – Ductal carcinoma in situ (CIS)
This duct exhibits a cribriform pattern but it also contains a central area of necrosis (arrow) representing comedonecrosis. No invasive component is present. |
|
|
Breast – Lobular carcinoma in situ (CIS)
Lobules are dilated and filled with a proliferation of bland monotonous appearing cells (arrows). |
|
|
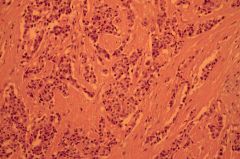
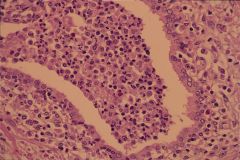
Breast – Infiltrating mammary carcinoma
Nests of small malignant epithelial cells infiltrating a dense desmoplastic stroma (the dense stroma is responding to the tumor). |
|
|
Mammogram of Cyst - Rounded mass with well circumscribed borders.
|
|
|
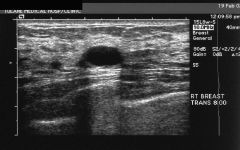
Simple Cyst of Breast - Ovoid mass which is anechoic, has well circumscribed margin, and demonstrates increased through transmission of sound deep to the mass (tissue is brighter deep to the mass).
|
|
|
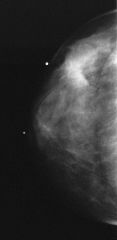
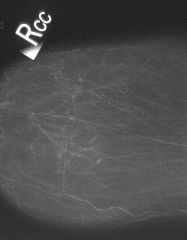
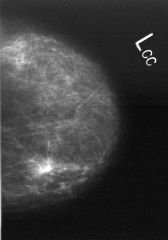
Infiltrating ductal carcinoma - Cranio-caudal view of right breast with BB marking a palpable lump (a second BB marks the nipple). Mammogram demonstrates an area of increased density with fine spiculations radiating from this mass at a corresponding location with subtle skin thickening also present.
|
|

|
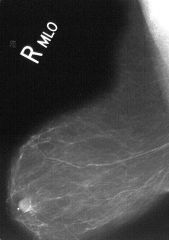
Infiltrating ductal carcinoma - Medial-Lateral Oblique view of right breast demonstrating similar findings.
|
|
|
Ductal carcinoma in situ - Cranio-caudal view of right breast demonstrationg clustered microcalcifications of varying sizes and shapes.
|
|
|
Ductal carcinoma in situ - Medial-lateral view of right breast demonstrating similar findings.
|
|

|
Ductal carcinoma in situ - Magnification view of microcalcifications suggests that some of these may be vascular in origin but others appear to be nonvascular and following a linear course (within the ductal system).
|
|
|
Papilloma - Craniocaudal view of left breast demonstrates several coarse calcifications in a focal area of increased density.
|
|

|
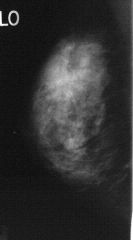
Fibroadenoma - Cranio-caudal view of the right breast demonstrates a round mass with well circumscribed borders.
|
|
|
Acute and chronic prostatitis - Prostatic gland contains intralumenal neutrophils, leukocytes, plasma cells, and histiocytes. Perglandular stoma contains chronic inflammatory cells.
|
|

|
Prostate – Benign Prostatic Hyperplasia (BPH)
An enlarged prostate, which on cut section, is represented by gray-white fibrous nodules. The nodules tend to protrude on cut section. Cancer is usually represented by soft nodules, which may shrink and appear umbilicated on cut section. Cancer may also be yellow in color. |
|

|
Prostate – Benign Prostatic Hyperplasia (BPH)
An enlarged prostate which on cut section, is represented by gray-white fibrous nodules. The nodules tend to protrude on cut section. Cancer is usually represented by soft nodules, which may shrink and appear umbilicated on cut section. Cancer may also be yellow in color. |
|

|
Prostate – BPH (micro)
Arrows surround a hyperplastic stromal nodule. This nodule is represented by hyperplastic fibroblasts and/or smooth muscle. |
|
|
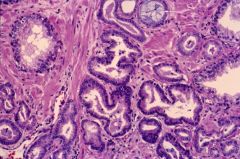
Prostate – BPH (micro)
Hyperplastic glands in BPH. The glands are lined by hyperplastic epithelial cells forming papillary aggregates (arrow) which grow into the lumen of the gland. |
|
|
Prostate - Adenocarcinoma
The prostate exhibits vague nodularity containing areas which are yellow in color (arrows). |
|

|
Prostate – Adenocarcinoma and BPH
Prostatic tissue on the right has nodularity (short arrows) representing BPH. The tissue on the left also exhibits multiple microcystic areas (small arrows) representing BPH. Long arrows point to more solid white tissue within the capsule representing adenocarcinoma. |
|

|
Prostate - Adenocarcinoma
Gray to white peripheral vague nodularity (arrows) represent adenocarcinoma. Note the central space representing the urethra and that the tumor is peripherally placed near the capsule. Most adenocarcinomas are peripherally located in the prostate. |
|
|
Prostate - Adenocarcinoma
Benign glands are present on top (short arrows). The small glandular structure contains nuclei with prominent nucleoli represent adenocarcinoma (long arrows). Adenocarcinoma of the prostate usually have prominent nucleoli. |
|
|
Prostate – Well differentiated adenocarcinoma
This tumor is low grade (Gleason’s-2) and is represented by well formed glands separated by fibrous stroma. The glands have pushing non-infiltrating margins. It is easy to see evidence of glandular differentiation in well differentiated adenocarcinoma. |
|
|
Prostate – Poorly differentiated adenocarcinoma
This tumor is high grade and is represented by small infiltrating malignant cells with little evidence of glandular differentiation (arrows). You do not see definitive glands here as you saw in the previous image representing well differentiated adenocarcinoma. |
|
|
Prostate - Adenocarcinoma
Prostate adenocarcinoma tends to invade nerves. This is an example of prostatic adenocarcinoma (long arrow) invading a nerve (short arrow). |
|
|
Prostate - Adenocarcinoma
Adenocarcinoma of the prostate tends to contain malignant glands which produce “blue mucin”. This is represented by intraluminal blue wispy amorphus material (arrow). |
|
|
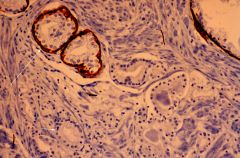
Prostate – High molecular weight cytokeratin
Benign and malignant glands Benign glands have a 2-cell layer lining. Malignant glands lack the second cell lining benign glands. This second cell lining benign glands expresses high molecular weight cytokeratin. The brown staining glands in this image are benign glands containing the second cell, which expresses high molecular weight cytokeratin (long arrows). The malignant glands do not express high molecular weight cytokeratin (short arrows). |
|
|
Prostate – High grade prostatic intraepithelial neoplasia (PIN)
High grade PIN has been associated with prostate adenocarcinoma. These ductular structures are lined by hyperplastic epithelial cells. Nuclei are hyperchromatic and contain prominent nucleoli, which are stratified. The basement membrane is intact. This could also be called severe dysplasia of this ductular structure. It is considered pre-malignant. |
|

|
Scrotum – Condyloma acuminatum
The scrotal skin contains multiple tan to pigmented sessile, cauliflower, papillomatous lesions representing condyloma acuminata. Histologically, these condyloma are similar to the ones seen in females. |
|
|
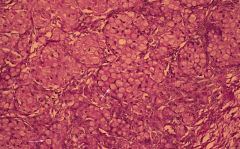
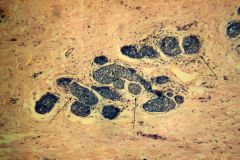
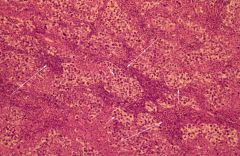
Testis - Seminoma
Nests of large polyhedral to round seminoma cells (short arrows), separated by delicate septa containing lymphocytic stroma (long arrows). |
|

|
Testis – Embryonal carcinoma
Testicular mass with central areas of necrosis and hemorrhage (arrow). Seminoma tends to be solid, fleshy, gray-white and without large areas of hemorrhage and necrosis. |
|

|
Hydrocele - transilluminated
This hydrocele sac has been trans-illuminated. The outer wall is thin and contains several dilated blood vessels. It would be fluctuant to palpation and when sectioned, it would reveal contents of straw to clear colored non-viscous fluid. |
|

|
Hydrocele
This hydrocele sae has been sectioned. It contains a smooth inner glistening surface (arrow). |
|

|
Spermatocele
Convoluted light gray glistening myxoid appearing cystic mass. Histologically spermatozoa would be found within this cyst. |
|

|
Penis – Giant condyloma
Cut section of penis containing a large tan cauliflower mass. |
|

|
Penis – Squamous cell carcinoma
This penis has been bisected longitudinally. It contains a white mass (arrow) which is arising in the distal urethra and is invading into the penis. Histologically it had features of a squamous cell carcinoma. |