Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
102 Cards in this Set
- Front
- Back
|
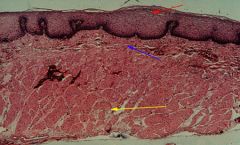
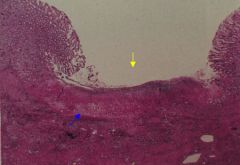
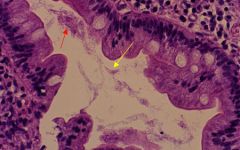
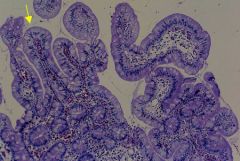
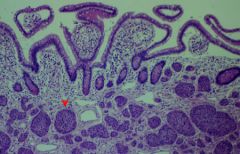
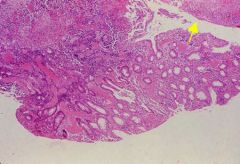
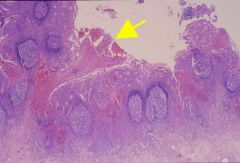
Normal Histology of the Esophagous: The esophagus is covered by nonkeratinized stratified squamous epithelium, the mucosa layer (red arrow). The submucosa (blue arrow) contains groups of small, mucus-secreting glands. The muscular layer (yellow arrow) consists of striated muscle at the proximal, smooth muscle at the distal end, and a mixture of the two muscle types in between.
|
|
|
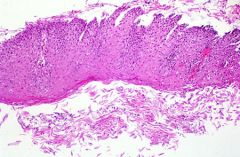
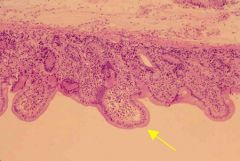
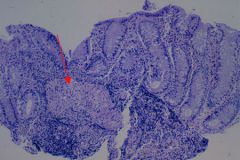
Hyperplastic squamous epithelium: Histologic section of the esophagous showing hyperplastic squamous epithelium with numerous denuded squamous epithelial cells in the luman. On H&E the appearance is that of reflux esophagitis.
|
|
|
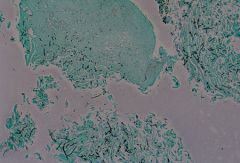
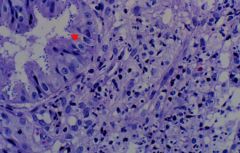
Candida esophagitis. A fungus stain showed the inflammation due to candida. Note the thick, black stained fungal forms.
|
|
|
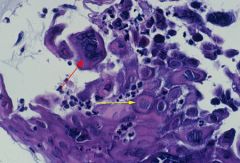
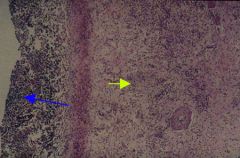
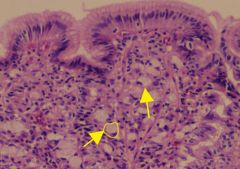
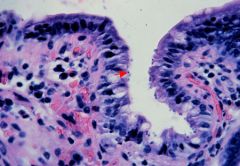
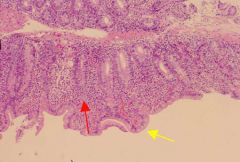
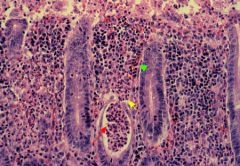
Herpes Esophagitis. Inflammation of the esophagous may be due to viruses such as herpes. Intranuclear inclusions are represented by ground glass nuclei (yellow arrow). Multi-nucleated forms with nuclear molding are also present (red arrow).
|
|
|
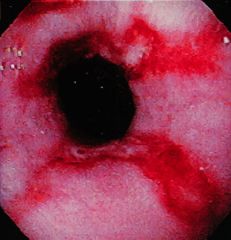
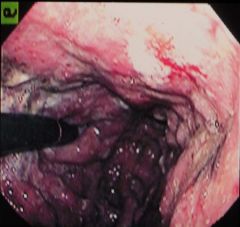
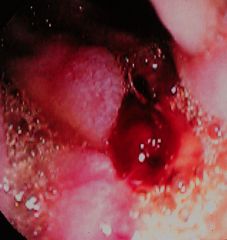
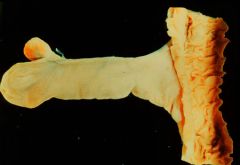
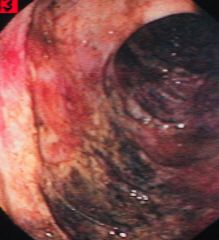
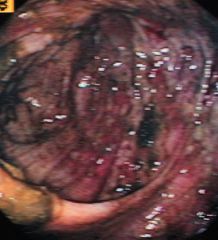
Reflux Espohagitis: Endoscopic appearance of reflux esophagitis showing tongues of red edematous mucosa extending upwards denoting areas of erosion.
|
|
|
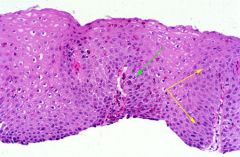
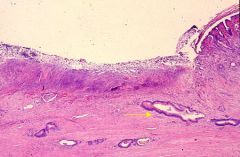
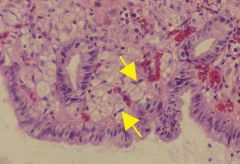
Histologic slide of reflux esophagitis. Note the elongation of dermal papillae reaching towards the surface (between yellow arrows). Note also the hyperplasia of the basal cells, and the presence of intraepithelial inflammatory cells (green arrow).
|
|
|
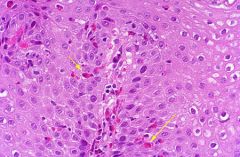
Close up view showing numerous eosinophils (yellow arrows) infiltrating the squamous mucosa. Eosinophils are indicators of reflux esophagitis.
|
|
|
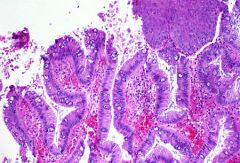
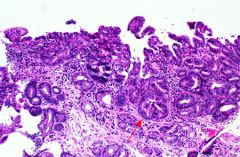
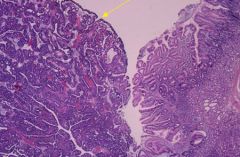
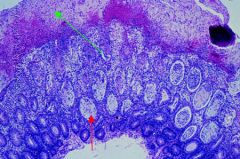
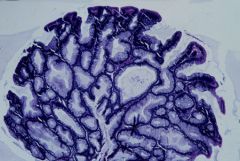
Histologic appearance of Barrett's esophagous. Note the presence of goblet cells and tall columnar epithelial cells. There is an island of residual squamous epithelium present in the upper right hand corner.
|
|
|
Metaplastic Barrett's epithelium with high grade dysplasia (red arrow).
|
|
|
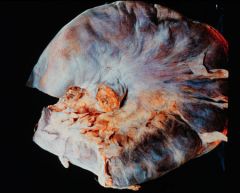
Carcinoma of the esophagous. A majority of such cancers are squamous cell carcinomas.
|
|

|
Carcinoma of the esophagous. A majority of such cancers are squamous cell carcinomas.
|
|
|
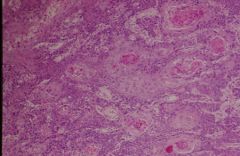
Histologic apperance of squamous cell carcinoma of the esophagous.
|
|
|
Histologic apperance of squamous cell carcinoma of the esophagous.
|
|

|
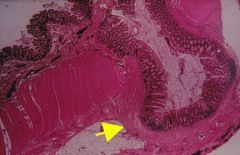
Mallory-Weiss tear (yellow arrow). Small, mucosal tears such as this sometimes occur near the esophagogastric junction following repeated vomiting, usually in an alcoholic. The histology (not shown) is of a nonspecific traumatic defect followed, if the patient survives, by an inflammatory response.
|
|
|
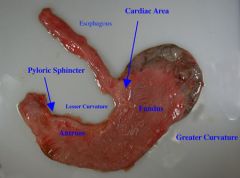
Normal Stomach
|
|

|
Endoscopic appearance of severe, nonspecific gastritis due to Helicobacter pylori. Note the edematous, red appearance of the gastric mucosa.
|
|
|
This is acute gastritis or the so-called acid indigestion, which is caused by irritating foods, over-ingestion of alcohol or aspirin or poisons. Here the mucosa is edematous and there are punctate submucosal hemorrhages.
|
|

|
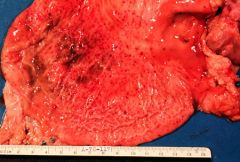
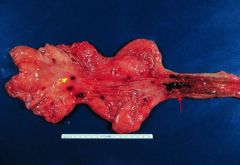
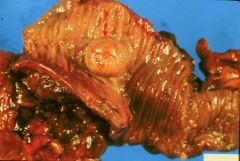
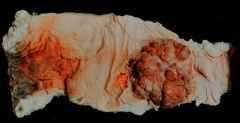
This is a stomach which has been opened along its greater curvature so that the lesser curvature is in the center of the specimen. Notice the rugae are almost completely lacking. This is chronic atrophic gastritis. It is associated with chronic alcoholism and with pernicious anemia. Typically these patients have achlorhydria and the incidence of cancer is increased three- fold in these patients, when they also find anti-parietal cell antibodies in the sera of such patients.
|
|
|
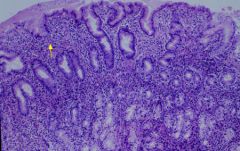
Chronic Gastritis. Numerous plasma cells and lymphocytes are present within the lamina propria (yellow arrow.)
|
|
|
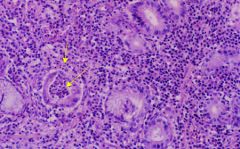
Histologic appearance of Helicobacter associated active gastritis. Note the neutrophilic infiltration of the lamina propria as well as neutrophils within glands (yellow arrows).
|
|
|
Hemorrhagic gastritis. Mucosa is markedly hyperemic and luminal surface contains attached blood clots. Not visibly apparent is an ulcer.
|
|
|
Acute gastric ulcers. Small, round, darkened areas with peripheral rims of hyperemia (yellow arrow). There are also areas of erosion in the distal esophagous (red arrow). When associated with increased intracranial pressure, such as trauma to the head, they are known as Cushing's ulcers. Similar type ulcers found in the proximal duodenum associated with burns or trauma are called Curling ulcers.
|
|

|
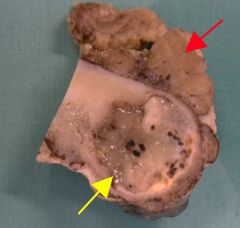
Chronic Gastric Ulcer: In sharp contrast to the small, multiple, superficial, acute gastric ulcers this is a chronic peptic ulcer lying in its characteristic location along the lesser curvature although its farther from the pylorus than usual. In the base of this ulcer is necrotic debris. Notice the smooth, rolled edges.
|
|

|
Stomach ulceration. Multiple dark areas represent mucosal defects or erosions (white arrow). Near the gastroduodenal junction is a benign ulcer represented by a punched out area with mucosal rugae extending up to the edge of the ulcer (yellow arrow).
|
|
|
Stomach with gastric ulcer
|
|
|
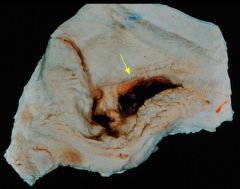
Mucosal Ulceration: A small, punched out area of mucosal ulceration (yellow arrow). Note smooth edges and rugae extending up to edge of the ulcer.
|
|
|
Stomach with gastric ulcer. There is a central defect represented by erosion of the mucosal surface (yellow arrow). The base of the ulcer is represented by fibrin and exudate (blue arrow).
|
|
|
Gastric ulcer- The inner luminal or mucosal surface is represented by a layer of necrotic tissue, and may have fibrinopurulent exudate (not shown here). Beneath this layer is a zone of inflammation that is predominantly neutrophilic (blue arrow). Chronically inflamed granulation tissue is beneath this layer (yellow arrow). A collagenous scar is ultimately produced by this layer.
|
|
|
Endoscopic appearance of gastric carcinoma. Note the heaped up margins of the tumor. It has a fungating cauliflower-like appearance.
|
|

|
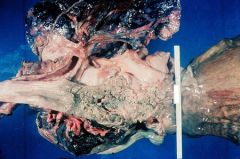
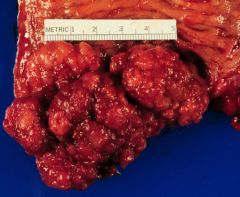
This is a carcinoma of the stomach. This is an 8 cm fungating lesion which extends into the lumen of the stomach. The ulcerating type of carcinoma is somewhat more common and then there is still a third type, the scirrhous or infiltrating type which causes the leather bottle stomach. These can occur anywhere in the stomach including the greater curvature which tends to differentiate them from gastric ulcers which occur only on the lesser curvature.
|
|

|
Stomach carcinoma, linnitus plastica type. A yellow arrow denotes a thickened wall. The mucosa has areas of hemorrhage, but is without a mass.
|
|

|
Gastric carcinoma. A fungating mass is shown by the yellow arrow.
|
|
|
Ulcerated adenocarcinoma. A yellow arrow points to malignant glandular structure with intestinal features.
|
|
|
Gastric carcinoma, signet ring cell type. Yellow arrows points to a classic "signet ring " cells. This is a large round cell with clear mucinous cytoplasm that causes the nucleus to be pushed to the edge of the cell. One cell is circled in yellow.
|
|
|
Gastric carcinoma, signet ring cell type. Yellow arrows points to a classic "signet ring " cells. This is a large round cell with clear mucinous cytoplasm that causes the nucleus to be pushed to the edge of the cell.
|
|
|
Histologic appearance of adenocarcinoma of the stomach (yellow arrow). The tumor has a complex glandular architecture of glands. Cells lining these glandular structures have malignant cytological features. Normal stomach is seen on the right.
|
|
|
Endoscopic appearance of bleeding duodenal ulcer.
|
|

|
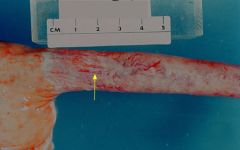
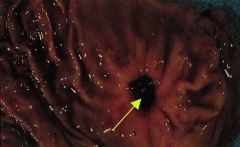
Duodenal ulcer -- Yellow arrow points to an oval ulcer with peripheral rim of hyperemia.
|
|
|
Duodenum, Giardiasis -- Yellow arrow depicts crescent shaped trophozoite, while the red arrow depicts a teardrop shaped trophozoite of giardia.
|
|
|
Cryptosporidiosis -- Small spherical organisms (red arrow) attached to the brush border of absorptive intestinal epithelial cells.
|
|
|
Cryptosporidiosis -- Small spherical organisms (red arrow) attached to the brush border of absorptive intestinal epithelial cells.
|
|

|
Pinworms: Colonoscopy, Enterobius Vermicularis (pinworms) -- Endoscopy reveals an area of mucosal erythema a white "s" shaped organism with features of e. vermicularis.
|
|
|
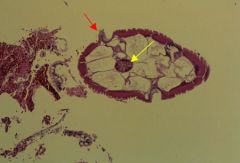
Pinworms (Enterobiasis vermicularis) -- Intestinal lumen containing a cross section of an adult e. vermicularis demonstrating a central intestine of the worm (yellow arrow) and lateral ala (red arrow).
|
|
|
Normal Small Intestine Mucosa. Villi are elongated and finger shaped (yellow arrow).
|
|
|
Abnormal small intestinal mucosa. Villli are short and flattened (yellow arrow). This is seen in malabsorption syndromes.
|
|
|
Small bowel, infectious enteritis. Villi are flat (yellow arrow) and the lamina propria contains numerous inflammatory cells (red arrow), predominately lymphocytes and plasma cells.
|
|
|
Meckel's Diverticulum -- A blind segment or outpocketing of the intestinal wall that includes all layer of the intestine.
|
|

|
Meckel's Diverticulum -- A blind segment or outpocketing of the intestinal wall. It includes all layer of the intestine: mucosa, submucosa, muscularis propria and serosa.
|
|
|
Ileum, carcinoid tumor -- Red arrow depicts a nodular tumor that is yellowish in color. Carcinoid tumors typically have a yellowish appearance.
|
|
|
Ileum, carcinoid tumor -- Multiple, small nests composed of small monotonous cells (arrow). The nests are separated by loose edematous connective tissue of the lamina propria.
|
|

|
Cecum (C) and ileum (I) - Crohn's Disease - the ileal mucosa is inflammed giving it a coblestone appearance. Note the uninvolved cecum (skip lesions).
|
|

|
Crohn's Disease - the lumen is stenotic and has the appearance of a garden hose. This would produce a "string sign " on barium enema.
|
|
|
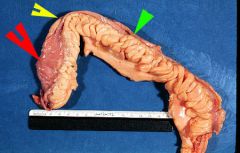
Crohn's Disease - On the left hand side, note essentially normal uninvolved segment (red arrow). Abruptly, the lumen becomes narrowed (yellow arrow) producing a stenotic segment of intestine similar to a garden hose. A barium enema would produce a "string sign". The mesenteric fat appears to be "creeping" around the antimesenteric serosal surface ("creeping fat")
|
|
|
Crohn's Disease - Section of colon exhibits increased numbers of lymphocytes and plasma cells. An aggregate of histiocytes is present forming a non-necrotizing granuloma (red arrow). There is acute cryptitis, and glandular regenerative hyperplasia present.
|
|

|
This is a classic example of chronic ulcerative colitis. Note the deep ulcer in the center, the cobblestone appearance of the mucosa, and the pseudo-polyps (yellow arrow). In addition to chronic hemorrhage and diarrhea, this condition is pre-malignant.
|
|

|
Ulcerative colitis gross - Hyperemia mucosa. There are irregular areas of ulceration which coalesce creating small islands of residual mucosa (pseudopolyp).
|
|
|
Ulcerative colitis, pseudopolyp - A polypoid area of mucosa is created by an active or acute inflammatory process. The inflammatory process causes mucosal ulceration (yellow arrow). The areas of ulceration surround viable mucsoa and interconnect leaving an island or polypoid shaped mucsoa known as a pseudopolyp.
|
|
|
Ulcerative colitis - The lamina propria contains increased numbers of plasma cells and lymphocytes. There are scattered eosinophils (green arrow) and neutrophils (yellow arrow) present as well. Centrally there is a crypt abscess (red arrow) represented by a gland lined by partially atrophic epithelium with intraluminal collection of neutrophils (microabscess). Other glands exhibit regenerative changes and prominent goblet cell depletion.
|
|
|
Pseudomembranous colitis - There are numerous ectatic crypts containing mucinous material and microabscesses (crypt abscesses)(red arrow). The surface of the mucosa contains mucinous fibropurulent exudate (green arrow), pseudomembrane. The lamina propria contains increased numbers of inflammatory cells.
|
|
|
Endoscopic appearance of ischemic bowel disease.
|
|
|
Endoscopic appearance of ischemic bowel disease.
|
|

|
Colon - hemorrhagic infarction
|
|

|
Colon - Acute Ischemic Colitis
|
|
|
Colonic volvulus - hemorrhagic infarction of colon.
|
|

|
Our major concern in the small intestine is obstruction, usually due to herniation, to adhesions, to volvulus or to intussusception. This is an example of intussusception in an infant, causing fatal obstruction. The invaginated segment is often infarcted due to compromised blood supply.
|
|

|
Diverticular disease involving the sigmoid colon. Note the diverticular opening in the mucosa (yellow arrow).
|
|

|
This is a case of diverticulitis of the sigmoid colon. There are numerous saccular protrusions from the colonic wall that pass through the muscularis.
|
|

|
Colon, Diverticulosis - There are multiple small spherical out pocketings of the mucosa extending through the wall of the colon into the serosa
|
|
|
Diverticulosis - there are numerous saccular protrusions (yellow arrow) of colonic mucosa extending throughthe muscularispropria of the colonic wall into the serosa.
|
|

|
This is the opened colon in a case of diverticulitis. The arrows point to ostia of the diverticula. These can become inflamed and produce fibrosing disease which can lead to obstruction. Also the vessels in the necks of these diverticula can cause massive GI hemorrhage.
|
|

|
Collagenous colitis - The biopsy reveals marked thickening of the basement membrane (yellow arrow) and increased numbers of lymphocytes and plasma cells within the lamina propria. Typically seen clinically with watery diarrhea.
|
|

|
Polyp in the colon
|
|

|
Polyp in the colon
|
|

|
Colonic ulcerated adenomatous polyp (blue arrow) and multiple other smaller adenomatous polyps (yellow arrows).
|
|
|
Colon - Tubulovillous adenoma - Villous and tubular shaped glands lined by adenomatous type epithelium forming a polyp.
|
|

|
Colon - Familial polyposis - there are numerous adenomatous polyps throughout the colon.
|
|

|
Colon - ulcerated adenocarcinoma represented by a round fungating mass (yellow arrow surround the tumor). Smaller blue arrow exhibits cut section of tumor.
|
|
|
Rectum - adenocarcinoma
|
|
|
Colon - adenocarcinoma
|
|
|
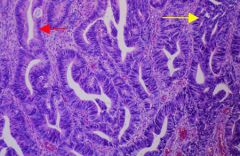
Colon - adenocarcinoma - Architecturally complex glands are lined by malignant glandular epithelial cells (yellow arrow). Red arrow exhibits a glandular structure which retains normal architecture but is still lined by malignant glandular epithelial cells.
|
|

|
This is a normal liver. Notice the dark reddish-brown color, the fine lobular texture, and the smooth capsular surface at the left. The first thing to notice when you observe the liver either at an autopsy or during an abdominal operation is its color.
|
|

|
Fatty liver. Notice its pale yellow color. It has a greasy feel to it and the cut surface tends to bulge. This is the early stage of alcoholic liver disease. It is also seen in nutritional deficiencies.
|
|

|
This is a bile stained liver of obstructive jaundice. Bile is backed up into all the bile ducts and into the bile canaliculi. There is increased portal markings probably due to periportal fibrosis.
|
|

|
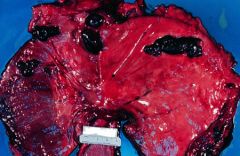
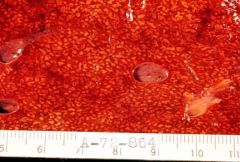
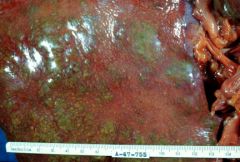
Chronic passive congestion: This is the classical nutmeg pattern seen in the cut section of liver, typical of chronic passive congestion. This is often seen in chronic congestive failure. The red markings are due to congestion and necrosis around the central veins of the lobules.
|
|

|
"Cardiac cirrhosis": After long-standing chronic passive congestion in chronic congestive failure there may actually be regeneration in the areas of central necrosis and fibrosis.
|
|

|
This is an example of pylephlebitis, literally an inflammation of the portal vein. Here bacteria have arrived in the liver by way of the portal system and you can seen small abscesses around the portal radicals particularly at the top of the specimen.
|
|

|
Perforated appendix with generalized peritonitis -- most common cause of pylephlebitis. The arrow at the bottom points to the perforation in the appendix and you can see a yellowish-green, fibrinous covering over the small intestines at the bottom of the specimen.
|
|
|
Here is an example of centrilobular necrosis the kind of necrosis that occurs after poisoning by organic solvents such as chloroform, trinitrotoluene and carbon tetrachloride. You will notice the centers of the lobules snow a yellowish coagulation necrosis. The centers of these areas of necrosis are often hemorrhagic.
|
|
|
Portal cirrhosis
|
|

|
On the cut section of Laennec's cirrhosis or portal cirrhosis notice again the fine nodularity on the cut surface. This specimen shows the tawny yellow color from which cirrhosis gets its name. The consistency of this liver is tough and fibrous, almost like leather. The great majority of cases of Laennec's cirrhosis have a history of high alcoholic intake. On the right is a so-called Zahn's infarct.
|
|
|
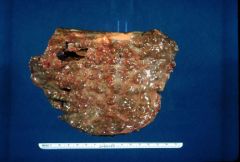
Here is a very different appearing cirrhosis. The nodules are variable in size measuring up to a centimeter in diameter. This is the typical post-necrotic cirrhosis or coarsely nodular cirrhosis. This occurs after hepatitis or liver poisoning. It results in either liver failure or in hepatome formation.
|
|

|
Post-necrotic cirrhosis, followed by viral hepatitis. Here the liver is severely distorted by regenerative nodules that are even larger than those in the previous case.
|
|

|
This is a fourth type of cirrhosis, biliary cirrhosis which follows biliary obstruction. In this case congenital biliary atresia. Here the liver is bile stained and there are fibrous strands extending out from the portal areas corresponding to fibrosis around bile ducts.
|
|

|
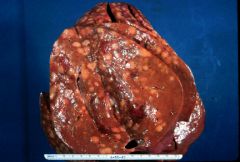
About five percent of all cases of cirrhosis develop malignant hepatoma, a primary tumor of liver which often takes this massive yellowish appearance. Pigment cirrhosis found in hemochromatosis and post-necrotic cirrhosis are most apt to develop malignant hepatoma.
|
|

|
Adenocarcinoma - most common malignancy of the liver. This is a well-defined adenocarcinoma which is metastasized from the colon by way of the portal vein.
|
|
|
Nodular Hodgkin's disease metastatic to liver.
|
|

|
Chronic lymphocytic leukemia. Remember that the sinusoids of the liver are part of the reticuloendothelial system and are commonly involved with leukemia as are the lymph nodes and spleen. Notice the pale, bulging surface.
|
|

|
Liver with a pale, bulging surface.Liver is filled with glycogen in von Gierke's disease, the glycogen storage disease of children.
|
|

|
Normal Appendix
|
|

|
Appendix, acute appendicitis - top image exhibits a fibrinopurulent exudate on the serosa (acute pertonitis). The bottom image exhibits fecoliths (red arrows) within the lumen. the wall of the appendix is thickened.
|
|
|
Acute appendicitis - there is luminal fibropurulent exudate with surface ulcerations (yellow arrow). Neutrophils should also be present in other layers of the appendiceal wall depending on the duration of inflammation (submucosa, muscularis propria, and serosa).
|
|
|
Appendix - mucinous cystadenoma - Distal tip of appendix contains a cystic tumor (yellow arrow) filled with mucinous material. Red arrow represents mesoappendix.
|