Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
24 Cards in this Set
- Front
- Back
|
Pheochromocytomas:
What are they? Cause |
Cathecholamine producing tumors
Arise from chromaffin cells of adrenal medulla or extra-adrenal paraganglia Most are adrenal in origin! adrenal origin = pheo extra-adrenal pheo = paraganglioma (15-20%) Cause: Sporadic Hereditary Syndromes |
|
|
Multiple Endocrine Neoplasia Type 2 is associated with ________ which results in _______.
|
RET proto-oncogene mutation, tyrosine kinase constantly active
|
|
|
MEN Type 2A vs 2B
|
2A: Medullary thyroid ca, pheochromocytoma, hyperpara
2B: medullary thyroid ca, pheochromocytoma, Marfanoid habitus, multiple neuromas |
|
|
Von Hippel-Lindau syndrome
What cancers is it associated with? |
Mutation in VLH tumor suppressor gene leads to pheo (addnly: RCC, retinal and CNS hemangioblastomas)
|
|
|
Neurofibromatosis type 1
|
Mutation of NF1 (tumor suppressor gene), manifests as cafe au lait spots, multiple fibromas on skin; only 5% have pheo
|
|
|
Familial paraganglioma
|
Mutation in succinate dehydrogenase enzyme complex (mitochondrial complex II) activates tumor-promoting genes
Manifestations: adrenal pheochromo, extra-adrenal pheo (paraganglioma), head and neck paraganglioma |
|
|
What is the rule of 10?
|
Sporadic pheos follow rule of 10:
10% hereditary 10% bilateral 10% extra-adrenal 10% malignant BUT IT'S NOT TRUE |
|
|
Triad of pheo symptoms.
Other symptoms. Include catecholamine effects. |
HA
Palpitations Sweating Which occur in spells (paroxysms) Hard to control HTN, HTN in paroxysms, orthostatic hypotn (catecholamine effects--vascularly constricted, volume depleted) Catecholamines inhibit insulin-->hypoglycemia |
|
|
Who should we test for pheo?
Tests used for screening? Include screening and confirmatory testing. |
Resistant HTN
Paroxysms suggestive of pheo Genetic risk factors (MEN2, ret mutation) Adrenal incidentaloma Screen for catecholamines or metabolites 24 hour urine collection, plasma metanephrines! Pheos continuously release metanephrines! very high sensitivity, but low specificity. needs confirmatory testing. Confirm with 24 hour urine collection for catecholamines and MN. |
|
|
What substances interfere with pheo testing?
|
Substances that rasise level of catechols or metabs or interfere with assay
Ex: Acetaminophen, antipsychotics, EtOH Coffee (even decaf) Labetalol, sotalol |
|
|
Clonidine Suppression Test:
Mechanism Use |
Clonidine (anti-HTN) suppresses catechol release
Catechols should go down If doesn't go down-->PHEO! |
|
|
Why should you NEVER run a glucagon stimulation test in someone with pheo?
|
glucagon causes NE levels to rise 3x in pheo, which can be FATAL
|
|
|
I123-MIBG Imaging
|
Pheo will uptake radiolabeled MIBG and will show up on CT/MRI
|
|
|
Pheo:
Pre-operative management - include dietary changes |
1) Alpha-blockade (phenoxybenzamine): may induce orthostatic hypotn, dizziness, syncope, congestion
If develop tachycardia, use beta-blockade (propanalol, atenelol) ALWAYS alpha block before beta block can also use Labetolol (combined alpha- and beta- blocker) 2) Salt loading (encourage high salt diet and liberal fluid intake while on phenoxybenzamine to reduce postop hypotn) |
|
|
Why should you administer alpha-blockade prior to beta-blockade?
|
Alpha effect-->vasoconstriction
Beta effect-->vasodilation If beta block first, unopposed alpha-adrenergic vasoconstriction can lead to hypertensive crisis |
|
|
Pheo:
Postoperative risks Prevention? |
Risk of HYPOtension:
Catecholamine levels fall alpha-blockade still active reduced with PRE-OPERATIVE VOLUME LOADING (give saline, high salt diet) Risk of hypoglycemia: Catechols suppress insulin secretion so after sx, insulin levels will rebound (give sugar? make sure they eat? didn't say.) |
|
|
Neuroendocrine Tumors:
Arise in the _____ |
throughout body
Arise in Resp Tract, pancreas, anywhere along GI tract (even appendix) May be fnal or nonfnal May arise sporadically or part of syndrome |
|
|
Multiple Endocrine Neoplasia Type 1:
Mutation Manifestations |
MEN type 1
Mutation on MENIN (tumor suppressor gene) Manifestations: Three P's hyperPARA Pituitary adenomas Pancreatic Neuroendocrine Tumors: gastrinoma (secrete gastrin), insulinoma (secrete insulin), nonfnal |
|
|
Carcinoid syndrome:
Due to Symptoms Circulation Pattern Testing |
Tumor secretion of 5-HT, vasoactive peptides (histamine, kallikreain, PGs)
Syx: FLUSHING Diarrhea Wheezing R-sided valvular heart dz Liver inactivates serotonin so carcinoid syndrome implues tumor effluent reaching systemic circulation without passing through liver (liver mets may drain into hepatic vein) Test: Urinary excretion of 5-HIAA (serotonin metabolite) |
|
|
VIPoma:
Symptoms |
Secretes vasoactive intestinal peptide
Syx: WDHA Syndrome Watery diarrhea hypokalemia achlorhydria (low stomach acid production) Test VIP level aka pancreatic cholera; Verner-Morrison syndrome |
|
|
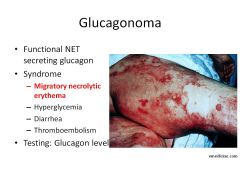
Glucagonoma:
Symptoms |
Syx:
Hyperglycemic migratory necrolytic erythema |
|
|
Somatostatinoma:
Symptoms Diagnostics |
Secretes SMS
Diabetes Gallblader Dz (inhibits gallbladder contraction) Diarrhea (same side effects as octreotide when treating acromegaly) Test: SMS level |
|

|
|
|
|

|