Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
37 Cards in this Set
- Front
- Back
|
What are hypersensitivity reactions?
Describe the 4 types. |
Hypersens Rxn: immune reactions that damage tissues of host
Type I (Ab-mediated; immediate): IgE binding to mast cells, basophils; re-exposure Type II (Ab-mediated; cytotoxic): IgG or IgM to fixed tissue Ag or Ag on cell surface Type III (Ab-mediated; immune complex): formation of immune complexes activate complement Type IV (CELL-MEDIATED; delayed): Ag-sensitized T cells release cytokines that attract macs to site of injury OR direct T cell mediated cytotoxicity (via CTLs) |
|
|
Describe the pre- and re-exposure phases of Type I hypersensitivity reactions.
|
Pre-exposure: IgE produced in response to antigenic stimulus; binds Fc receptors on mast cells
Dendritic Cells capture Ag (DC's are everywhere in body) Process, present via MHC II Present to naive T cells Dx/Dy to Th2 Produce Cytokines Activate B cells-->class switching to produce IgE plasma cells 2) Re-exposure to Ag: Mast cell degranulation-->syx Re-exposure to same Ag (or cross-reactive Ag) causes CROSS-LINKING of IgE RECEPTORS of MAST CELLS Discharge pre-formed granules and secondary mediators (latter requires synthesis) |
|
|
What cytokines do Th2 cells release to ensure IgE production and survival of eosinophils?
|
IL-4, -13: Turn on IgE producing B cells
IL-3, 5, GM-CSF: Survival of eosinophils |
|
|
What pre-formed granules are released by mast cells? What are their effects?
What secondary mediators are released by mast cells? What are their effects? |
Histamine: inc'd vasc perm, vasodil, bronchoconstriction, mucous secretion
Proteases, acid hydrolases: cleave complement, degrade BV BM and microbes Chemokines (ECF, NCF): attract nphils TNF: upregulate adhesion molecs Secondary: NEWLY SYNTHESIZED LIPID MEDIATORS: Leukotrienes C4 AND D4: inc'd vasc perm, bronch smooth muscle contraction (MOST VASOACTIVE AND SPASMOGENIC SUBSTANCES KNOWN) Leuk-B4: chemokine PAF: inc'd vasc perm, vasodil, platelet agg, histamine release Cytokines: TNF: upregulate adhesion molecs IL-3, 5, GM-CSF: activate eosinophils and promote survival IL-4: Th2 dx/dy |
|
|
How does the late phase reaction of type I hypersensitivity reactions occur?
What is the purpose of this response? Are antibodies required? |
Intense infiltration of tissues with eosinophils (destroy parasites AND host tissue AND induce inflammn), nphils, bphils, monocytes, and CD4+ T cells
In cases of allergic rhinitis and bronchial asthma, results in mucosal epithelial damage Recruited cellular infiltrate serves to AMPLIFY inflammatory response and doesn't require presence of Ag (tx with steroids may be necessary) |
|
|
What do eosinophils release? Effects?
|
Toxic Proteins:
Major Basic Protein (toxic to parasites and mammalian cells; triggers histamine release) Eosinophil cationic Protein (toxic to parasites) Enzymes Cytokines Lipid meds |
|
|
Describe consequences of:
Food allergy ingestion Inhalation of low dose antigen into upper airways Inhalation of allergen into lower airways |
Ingestion: GI mucosal IgE mast cell degranulation (can cause vomiting bc of smooth muscle contraction, if Ag diffuses into blood, can result in systemic syx)
Inhalation: Upper Airways: allergic rhinitis and conjunctivitis (hayfever) Lower Airways: Allergic asthma (70% of asthma is IgE mediated!!) |
|
|
Describe the progression of acute asthma to chronic asthma.
Discuss neuronal reflex. |
Acute: bronchoconstriction, occlusion of bronchi with mucous plugs (mucous hypersecretion)
Mast cell mediators result in influx of inflamm cells and increased ephil activtn Ephil degran causes tissue injury and entry of more inflamm cells Epithelial cell injury stimulates nerve endings Results in NEURONAL reflex Contributes to airway narrowing and mucus secretion Result is chronic inflammation (characterized by reversible narrowing of airways with wheezing, SOB, coughing) |
|
|
What kinds of antigens can trigger asthma?
|
Antigens that favor production of Ag = ALLERGENS
Small, highly soluble proteins on particles such as pollen or mite feces CAN DIFFUSE INTO MUCOSA |
|
|
What is the major allergen in the feces of house dust mites?
|
Der p 1 (a cysteine protease that cleaves occludin in tight jns)
|
|
|
What is wheal and flare?
|
When subcutaenous low dose ag is injected and results in local release of histamine.
Wheal = center of lump Flare = skirts of wheal Occurs 5-10 mins post administration |
|
|
Three ways to determine what someone is allergic to.
|
1) History
2) Skin test (wheal and flare) 3) RAST (radioallergosorbent testing): measure of specific serum IgE ab's |
|
|
What does it mean if someone is atopic?
What is the atopic triad? |
Prone to produce IgE ab's in response to various Ag's; have strong immediate hypersensitivity responses
Genetic tendency to have hypersensitivity Atopic Triad: -Allergic rhinitis (hayfever) -Asthma -Atopic dermatitis (eczema) or urticaria/hives |
|
|
Describe the two mechanisms by which type II hypersensitivity reactions occur.
|
1) Direct lysis: IgM or IgG react w/ag on cell surface and results in complement activation-->MAC
(ex: ABO mismatch-->lysis of transfused RBCs) 2) Opsonization: cells susceptible to phag by fixation of Ab (IgG or IgM) or C3b frag to cell surface |
|
|
ABO mismatch is an example of a _________ type II reaction.
|
Direct Lysis
|
|
|
Erythroblastosis fetalis is an example of a __________ type II reaction.
|
Opsonization
|
|
|
How can erythroblastosis fetalis be avoided?
|
Treatment at time of delivery with RhoGAM (anti-Rh gamma globulin)
RhoGAM contains Ab's against Rh+ rbc's and destroys them before maternal bloodstream can react by producing its own anti-Rh ab's |
|
|
A+ vs A-: Antigens Present
|
A+: Antigen A and Rh (D antigen)
A-: Antigen A |
|
|
How do autoimmune cytopenias occur?
|
Individuals produce Ab's to their own blood cells
|
|
|
How does drug-induced reaction occur?
|
Nonspecific adsorption and firm attachment of a drug onto RBC surface; drug is not immunogenic; it's a hapten (can induce an immune response when bound to cell)
|
|
|
How does complement result in inflammation?
|
Deposited Abs in BM, matrix activate complement by binding of Fc receptor on cell surface
C5a/3a recruit nphils and monos Activate Leuks Release enzymes, ROS TISSUE DAMAGE |
|
|
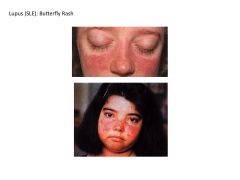
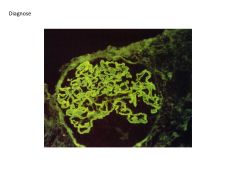
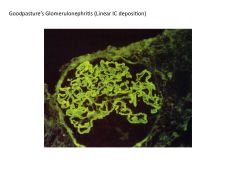
What is anti-glomerular basement membrane nephritis?
What other disease is it associated with? Defining characteristic of this disease? |
Dz where autoab's directed against normal components of Glomerular BM and result in rapidly progressive renal failure
When cross-react with other BM's (such as in lung) can result in pulmonary lesions (necrotizing hemorrhagic interstitial pneumonia) --GOODPASTURE syndrome Defining characteristic of goodpasture = linear deposition of autoab's |
|
|
How does antibody-dependent cellular cytotoxicity arise? What pathology is it associated with?
|
NK cells, nphils, ephils, macs bind Fc portion of Ab bound to target cell
NK cells and ephils inject perforin Macs and nphils release granzymes and TNF NO COMPLEMENT INVOLVEMENT May be involved with: Autoimmune Thyroiditis |
|
|
What is antibody-mediated cellular dysfunction? Examples?
|
Ab binding specific target cell receptor doesn't lead to cell death but to change in fn without cell injury or inflammn
Myasthenia Gravis: Ab blocking of receptor-->muscle weakness Graves Dz: Ab to TSH receptor results in stimulation of receptor |
|
|
How to Type III hypersensitivity reactions occur?
How do they result in tissue damage? Can this damage ever be extravascular? |
Type III = Immune Complex reaction
Formation of circulating Ag-Ab complexes that deposit in vessel walls and activate complement Formation of Ag-specific Ab's. As more and more Ag-Ab complexes form, some bind inflamm cells vis Fc or C3b (!!!) receptors, trigger vasoactive mediator release Inc'd vasc perm Deposition of immune complexes in vessel walls WBC recruitment (nphils) and results in inflammation (tissue damage bc of lysozymes) Can be systemic or localized Can be extravascular if antigen is planted extravascularly |
|
|
What is serum sickness?
Symptoms? Acute vs Chronic Serum Sickness |
When patient produces ab's to foreign (horse for ex.) serum proteins
Ab's form Ag-Ab complexes with Immune complex deposition results in symptoms Syx: Joint inflammation (arthritis, arthralgia) Skin rash (urticaria) Fever Glomerulonephritis Acute: single large exposure to Ag, lesions tend to resolve Chronic: repeated or prolonged exposure to antigen |
|
|
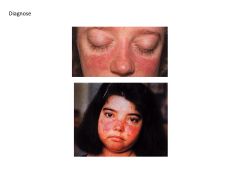
what is systemic lupus erythematosis?
Requirement for diagnosis? Symptoms? Most commonly involved organ? |
Chronic autoimmune microvascular inflamm disease that can affect EVERY ORGAN
Due to production of auto-Ab's to NUCLEAR Ag's Ab's to dsDNA specific for dx of SLE Syx: Skin Rashes (BUTTERFLY RASH) Arthritis Glomerulonephritis Remember signs and syx are MULTI-SYSTEM in nature: fever, fatigue, weight loss Arthritis, myalgia Photosensitivity, malar rash, alopecia Seizures Penumonitis KIDNEY IS MOST COMMONLY INVOLVED VISCERAL ORGAN |
|
|
Glomerulonephritis: SLE vs Goodpasture's Syndrome
|
SLE:
Course, granular deposition of immune complexes, Type III hypersensitivity reaction Goodpastures's: Linear deposition of immune complexes |
|
|
Does the formation of antigen-antibody complexes in circulation always imply the presence of disease?
|
No, ag-ab complexes produced during normal immune response, normally cleared by phagocytic system.
Excessive production of immune complexes can overwhelm phagocytic system and result in tissue damage |
|
|
What determines the extent of immune complex deposition?
|
Size!
Larger complexes are rapidly removed within minutes by liver Smaller complexes circulate for longer periods |
|
|
Arthus Reaction vs Wheal and Flare
|
Arthus: Type III, IC-mediated
Peak in 4-10 hours (initiated by injecting Ag into previously exposed animal and results in LOCAL formation of IC's resulting in localized tissue necrosis) Ex: local reaction to tetanus booster Wheal and Flare: Type I, IgE mediated, appears immediately |
|
|
|
|

|

|
|
|
|
|
|
What is a Type IV hypersensitivity reaction?
Describe the 2 subtypes. |
Cell-Mediated immune response with sensitized T lymphocytes involved
AKA Delayed Hyperensitivity NO AB INVOLVEMENT 1) Delayed-Type: ex: host response to Tb; ppd Upon first exposure to mycobact tb, macs phag and attempt kill Mycobact replicate in phagolysosomes Macs overwhelmed Process, present Ag via MHC II, call in CD4's (via IL-12!) Expansion of Th1's to rev up macs Mounted Th1 response (takes 3 weeks) Injury caused by T cells, macs (granuloma formation) 2) Cell-Mediated Cytotoxicity: killing of Ag-bearing target cells by cytotoxic T lymphocytes (CD8+ T cells) CTL's actvd by Class I MHC (major defense against intracellular infections) CTL's lead to tissue injury by killing infected cells even if virus has no cytopathic effects (as with HBV) Injury results from perforin + granyzme mediated killing OR by Fas-Fas ligand-dependent killing |
|
|
Does a positive ppd mean someone has active TB?
Why is a positive result indurated? Why should elderly patients receive a two-step ppd? |
No, means that the person ahs been exposed to Tb at some point and has mounted an ag-specific Th1 reaction
May be at risk of re-activation of TB at later time unless receive tx Accumulation of mononuclear cells (mostly CD4_ and increased microvasc perm means escape of plasma prots (edema and induration) Initial negative ppd in an elderly person who had been exposed to TB as child may be a WANING TH1 RESPONSE Repeat ppd 1-3 weeks later may be positive because of a boosted Th1 response (memory response to previously act'd Th1's) |
|
|
Use poison ivy to describe contact dermatitis.
What subclass of Type IV reaction is this? |
Upon re-exposure to poison ivy antigen (urshiol)
Urshiol serves as hapten (not capable of mounting an immune response until it reacts with skin proteins to become an antigen) Epidermal blister is result of Th1 accumulation and release of cytokines that cause damage to keratinocytes, causing cell separation and infiltration This is DELAYED-TYPE HYPERSENSITIVITY |