Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
74 Cards in this Set
- Front
- Back
|
Know the definition for anemia
|
reduction of hemoglobin concentration in blood and/or RBC count
Anemia is not a diagnosis, it is a manifestation of an underlying disorder |
|
|
Understand the general causes of anemia and consequence/symptoms
|
Causes
-Excessive destruction of red blood cells -Blood loss -Inadequate production of red blood cells Acute onset: rapid heartbeat lightheadedness shortness of breath Chronic: irritability, fatigue, weakness headache, vertigo pallor of mucous membrane (e.g. under eye), skin color is less reliable sensitivity to cold loss of appetite Sxs: |
|
|
How do adaptations that occur mask anemia?
|
SPEED OF ONSET: Rapid onset causes more symptoms (less time for adaptation)
SEVERITY: Mild anemia often no symptoms AGE: Anemia is less well tolerated by elderly (cardiovascular compensation impaired); however, very common among elderly Hb O2 DISSASSOC CURVE: Rise in 2,3 BPG (2,3-Bisphosphoglycerate) yields in more oxygen released |
|
|
Know what: Hct, Hgb, and RBC tests mean.
|
Hct (hematocrit) = percent volume of blood contributed by red blood cells
Hgb = total Hb RBC = RBC count |
|
|
7. Understand what red blood cell indices are.
|
REALIZE THESE ARE PER-CELL CALCULATIONS
Measures hemoglobin volume/concentration and red blood cell size. The relationships between the hematocrit, the hemoglobin level, and the RBC are converted to red blood cell indices through mathematical formulas. |
|
|
Define mean corpuscular hemoglobin (MCH)
What do we call low, normal, and high hemoglobin levels? what's the eqn for MCH? |
amount of hemoglobin per red blood cell.
Hgb/RBC hypochromic anemia: MCH low normochromic anemia: MCH normal hyperchromic anemia: MCH high |
|
|
9. Define Mean corpuscular hemoglobin concentration (MCHC)
|
calculation of the concentration of hemoglobin inside the red blood cells (takes size into account)
Hgb/Hct |
|
|
Define mean corpuscular volume (MCV)
What do we call low, normal, and high volume levels? what's the eqn for MCV? |
10. Define mean corpuscular volume (MCV)
average single red blood cell size Hct/RBC normocytic anemia: MCV normal microcytic anemia: MCV low macrocytic anemia: MCV high |
|
|
What type of anemia (red blood cell indices) would you expect in thalassemia? Explain why
|
Hypochromic, microcytic anemia (low MCH, low MCV)
Understand that b-thalasemia cells have less Hb and are this affects RBC development = smaller cell. |
|
|
Understand the different clinical aspects/techniques used to look at anemia (what are they, what do they look for, and what does it determine?)
|
1. ANALYZER:
hematocrit (Hct) = packed RBC volume (percent blood vol made up of RBCs) total hemoglobin (Hgb) = total Hb number of red blood cells = #RBCs 2. CALCULATE RBC INDECES red blood cell indices (MCH and MCV) i. Mean Corpuscular Volume 1. normocytic anemia: MCV normal 2. microcytic anemia: MCV low 3. macrocytic anemia: MCV high ii. Mean Corpuscular Hb 1. normochromic anemia: MCH normal 2. hypochromic anemia: MCH low 3. hyperchromic anemia: MCH high MICROSCOPY of BLOOD FILM 1. sickles - SCA 2. pencil shapes - FE deficiency WHOLE BLOOD CELL EVALUATION 1. Includes leukocyte (white blood cell) and platelet counts: 2. Helps to distinguish “pure” anemia from pancytopenia (drop in number of all blood cells) 3. If all cell numbers are low: marrow hypoplasia or infiltration, general destruction of cells (e.g. hypersplenism) 4. If leukocytes and platelet count is high: infections, leukemias, hemolysis, hemorrhage RETICULOCYTE COUNT immature RBCs - meas of how fast RBCs are made i. The reticulocyte count rises when there is a lot of blood loss or in certain diseases or where red blood cells are destroyed prematurely, such as hemolytic anemia. BONE MARROW EXAM Aspiration: liquid of bone marrow. Morphological information on developing cells (more information on hematopoiesis) Trephine biopsy: solid cores of bone marrow which is examined microscopically (sometimes with the aid of immunohistochemistry) for cellularity and infiltrative processes. |
|
|
Define whole blood cell evaluation.
What do we use it for? What does it mean if all cell numbers are low? What does it mean if leukocytes and platelets are high? What do high |
1. Includes leukocyte (white blood cell) and platelet counts:
2. Helps to distinguish “pure” anemia from pancytopenia (drop in number of all blood cells) 3. If all cell numbers are low: marrow hypoplasia or infiltration, general destruction of cells (e.g. hypersplenism) 4. If leukocytes and platelet count is high: infections, leukemias, hemolysis, hemorrhage |
|
|
What is microscopy?
What diseases can we identify using it? (there may be more than what I have here) |
Microscopy = analysis of blood film (microscopy)
1. sickles = sickle cell anemia 2. pencil shapes = Fe deficiency |
|
|
What does a reticulocyte count help us determine?
|
The reticulocyte count rises when there is a lot of blood loss or in certain diseases or where red blood cells are destroyed prematurely, such as hemolytic anemia.
|
|
|
Name and describe the (2) types of bone marrow exams.
|
i. ASPIRATION: liquid of bone marrow
Morphological information on developing cells (more information on hematopoiesis) ii. TREPHINE BIOPSY: solid cores of bone marrow which is examined microscopically (sometimes with the aid of immunohistochemistry) for cellularity and infiltrative processes. FYI-Blood Panel |
|
|
Know that... anemia is the most common anemia. What is the consequence for the synthesis of heme and hemoglobin, what is the consequence for the red blood cell size?
|
Iron deficiency (sideropenic anemia)
microcytic |
|
|
What are the possible causes of iron deficiency and what is the treatment?
|
What are the possible causes of iron deficiency and what is the treatment?
Causes loss of blood (including from heavy menstrual bleeding, ulcers, pregnancy, nursingdiet low in iron poor absorption of iron Treatment:Oral iron supplements (ferrous (Fe2+) sulfate), in extreme cases, parenteral |
|
|
Explain the iron cycle in the body:
|
b. Absorption of dietary iron as either:
i. iron (transporter DMT-1) ii. Intact heme (transporter HCP-1) (digested to release Fe) c. Transferrin xports Fe to marrow cell (free Fe is toxic!) i. Ferritin stores Fe ("ferret it away") ii. Neg-fb, if XS Fe (no xferrin receptor made) d. Delivered to mitochondria & incorporated into heme e. Heme combines with globin chains (a2b2) to form hemoglobin f. Circulation of Fe g. Some secretion, mostly recycling of Fe after RBC destroyed |
|
|
Know that. . . is the most commonly used as diagnostic tool to measure iron levels in body
|
a. SERUM FERRITIN - Amt of ferritin rel into blood is prop to amt of tot Fe stored
|
|
|
How does iron overload (hemochromatosis) occur and why is this a problem?
|
No physiological mechanism for XS Fe elimination (e.g. thalassemia victims get xfusions but can't get rid of XS iron)
Overload: Damage to organs, especially heart, liver, endocrine organs Abnormal deposition of an iron-containing compound (hemosiderin) in tissues Usually caused by genetic disease (common ~1/300): HFE (HEMOCHROMATOSIS) gene (iron absorption & regulation) |
|
|
What type of anemia (red blood cell indices) does iron deficiency cause?
|
Hypochromic, microcytic anemia
|
|
|
What could cause high Fe levels?
|
HFE (hemochromatosis) gene (Fe abs + reg)
Resulting in Organ damage (heart, liver, endocrine) and/or abnormal deposit of Fe in tissues |
|
|
Which proteins transport and store iron in the body?
|
Xferrin, ferretin
|
|
|
What are the treatments for Fe overdose?
|
phlebotomy or iron chelating therapy
|
|
|
What do thalassemia and iron deficiency anemia have in common?
|
Result in smaller, less numerous RBC's: hypochromic (MCH), hypovolemic (MCV).
|
|
|
briefly describe sideroblastic anemia
|
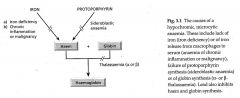
Failure of protoporphyrin synthesis due to a lack of Fe (usually)
|
|
|
Describe lead poisoning
|
Lead poisoning inhibits both HEME --AND-- GLOBIN synthesis Interferes with ALAD, zinc binding protein impt in syth of hemeInterferes w/ferrochelatase which catalyzes binding of protoporphrin and Fe2+ to form hemeResult: microcytic, hypchromic anemia
|
|
|
Be able to explain why iron deficiency, sideroblastic anemia, thalassemia, and lead poisoning cause microcytic, hypochromic anemia.
|
all three of these retard hemoglobin synthesis. Hb is necessary for proper RBC development, as a result cells are small (microcytic) and have less Hb (hypochromic)
|
|
|
Describe sideroblastic anemia
|
Genetic or acquired cause leading to Fe deficiency; Adequate iron but unable to incorporate iron into hemoglobin (protoporphoryn synthesis). Iron accumulates in mitochondria of erythroblasts in bone marrow.
|
|
|
Understand that ____ and vitamin ____ deficiencies are common causes for megaloblastic anemias. What is the molecular basis for this?
|
folate , B12Folic acid (Vitamin B9):Required for several steps of DNA synthesisVitamin B12:Required to convert methyltetrahydrofolate into tetrahydrofolate
|
|
|
Be able to briefly outline vitamin B12 absorption.
|
meat is best source (not in plants) initially binds to salivary R-protein vitamin B12 then binds to intrinsic factor (IF) in stomach uptake of B12-IF across intestinal wall into circulationtranscobalamin II xports to marrowstored in liver
|
|
|
Know what causes pernicious anemia. Understand the main causes for vitamin B12 deficiencies.
|
pernicious anemia: autoimmune destruction of gastric parietal cells, lack of IF production = B12 deficiency (can't absorb)
Causes congenital lack or abnormality of intrinsic factortotal or partial gastrectomy Intestinal causes -Crohn’s disease -Surgical removal of intestine or part of it -Stagnant loop syndrome (obstruction of part of intestine, bacterial overgrowth) -chronicle tropical sprue (malabsorption disease caused by infections) -fish tapeworm |
|
|
What are the main causes for folate deficiencies?
|
Excess utilization
-increased need during pregnancy (dividing cells), lactation -hematological or malignant diseases -inflammatory diseases Nutritional -poor diet, famine, old age Intestinal causes -Crohn’s disease surgical -removel of intestine or part of it -stagnant loop syndrome (obstruction of part of intestine, bacterial overgrowth) -chronical tropical sprue (malabsorption disease caused by infections) |
|
|
What are the treatments for folate and vitamin B12 deficiencies?
|
Folate = folic acid, PO, 5mg
B12 = hydroxycobalamin, IM, 1000ug |
|
|
What is the definition for hemolytic anemia?
|
anemias that result from an increase in red blood cell destruction
|
|
|
Know how red blood cells are normally disposed of. What organ is most important and what cell type removes the RBC's? What other organs besides the major one can perform this task?
|
Removed by macrophages of the reticuloendothelial system in spleen, liver, marrow
|
|
|
Be able to list and briefly define the three main genetic defects for intrinsic anemia.
|
Membrane-hereditary spherocytosis, elliptocytosis
Metabolism-G6PD deficiency, pyruvate kinase deficiency Hemoglobin-genetic abnormalities (sickle cell anemia, thalassemia) |
|
|
Be able to LIST the two cases of red blood cell membrane disorders. Why do they cause hemolytic anemia?
|
Spherocytosis and elliptocytosis
sphere shaped rather than doughnut shaped Diag by microscopy |
|
|
Be able to briefly describe G6PD (Glucose-6-phosphate dehydrogenase) deficiency (molecular cause, metabolic problem).
|
pentose-phosphate pathway - gens NADPHgens reduced glutathione, to defend vs oxidative stress reduce Fe3+ to Fe2+)Deficiency renders cell susceptible to oxidative stress
|
|
|
Why is this G6PD deficiency -based anemia such a problem for the use of anti-malaria drugs?
|
Antimalarials like primaquine: mechanism of action not well understood but they may produce reactive oxygen species…this is what's causing our hemolytic crisis to begin w
|
|
|
Be able to very briefly define pyruvate kinase deficiency.
|
Metab defect, Reduction in ATP generation:pyruvate kinase: phosphoenolpyruvate to pyruvate
RIGID, RBCs as result of ATP lack |
|
|
How does the malaria parasite cause hemolytic anemia?
|
Plasmodium invades, multiplies in and destroys red blood cells, Hemoglobin used as nutrient source by parasite
|
|
|
Know what chronic anemia is.
|
Repetitive, long-lasting anemias, usually disease caused
ommon causes Chronic infections Tuberculosis HIV Osteomyelitis Chronic inflammation (e.g. rheumatoid arthritis, systemic lupus erythematosus, chronic inflammatory liver diseases) Malignancies (carcinoma, lymphoma, leukemia) |
|
|
Be able to describe aplastic anemia. Understand how serious this type of anemia is.
|
Bone marrow does not prod enough blood cells (total blood cells not just red)Leads to rapid death <6mos
|
|
|
Know what primary and secondary polycythemia (erythrocytosis) is.
|
Polycythemia (erythrocytosis): overproduction of red blood cells
Primary polycythemia: no increase in erythropoietin, myeloproliferative disease (polycythaemia ruba vera) Secondary polycythemia: increase in erythropoietin (tumors, low oxygen levels, heart disease, heavy smoking, kidney disease) |
|
|
Categorize the following anemias
hemolytic anemia pernicious anemia lead poisoning alcohol, liver disease anemias of chronic disease sideroblastic anemia myelodysplasia thalassemias renal disease acute hemorrhage folate deficiency |
NN: decr #rbc but normal size and Hb content
HypoMicro: anything affecting Hb development = retard cell dev HyperMicro: Lg size, little replication chromic/cytic hemolytic anemia - N/N pernicious anemia - N/Mac lead poisoning - Hypo/Mic alcohol, liver disease - N/Mac anemias of chronic disease - N/N sideroblastic anemia - Hypo/Micro ---------------------------------- myelodysplasia - N/Macro ---------------------------------- thalassemias - Hypo/Micro renal disease - NN acute hemorrhage - NN folate deficiency - N/Macro |
|
|
What test do we use to ID microcytic hypochromic anemia?
|
serum ferrtin most common
Lead poisening Thalassemia Sideroblastic anemia Vitamin deficiencies: Lack of transferrin due to vitamin A (pyridoxine) deficiency Lack of heme synthesis due to B6 deficiency |
|
|
Describe megaloblastic anemia and how we test for it.
|
Megaloblastic (macrocytic) anemia - cell grows but doesn't divide, prob w/dna synth (high MCV + direct meas of folate/b12)
Vitamin B12: direct measurement of serum B12 levels measurement of homocysteine or methylmalonic acid serum levels shilling test (absorption test using radioactive B12) IF and gastric parietal cell antibodies Folate: serum folate levels red blood cell folate levels |
|
|
Effects of megaloblastic anemia
|
Effects:Resulting in unbalanced cell growth, impaired cell division
Mature cytoplasm, immature nucleus, larger cell volume Large but less red blood cells produced |
|
|
Causes of megaloblastic anemia
|
Vitamin B12 deficiency
Folate deficiency Other defects of DNA synthesis |
|
|
Why would you give vitamin B12 as an injection and not orally?
|
Pt missing part of stomachPernicious anemia = no IF, thus can't abs through stomach = need iv
|
|
|
What type of anemia (red blood cell indices) would occur in hemolytic anemia?
|
normocytic, normochromic
|
|
|
Could thalassemia or sickle cell anemia lead to hemolytic anemia?
|
SHAPE is critical!Sickle cell: RBCs are shaped strangely = identified by macrohages and destroyedExcess of a-chains precipitate = change in RBC structure and thus shorter lifespan
|
|
|
What causes elliptocytosis and spherocytosis
|
RBC membr disorder = eliptica/sphere shape vs donut
|
|
|
What metabolic pathway is affected in G6PD deficiency and why does that cause hemolytic anemia?
|
PPP pathway, oxidative stress
|
|
|
What is the difference between intrinsic and extrinsic hemolytic anemia?
|
Genetic vs acquired (malaria)
Infections Autoimmune disorders Some medications |
|
|
Anemia can be difficult to identify because:
Early symptoms may be mild Early on, it is not symptomatic There are no definite tests to confirm the condition All of the above |
early symptoms may be mild
|
|
|
What tests are used in the diagnosis of anemia?
a. White blood cell (WBC) count b. Hemoglobin c. Hematocrit d. Red blood cell (RBC) count e. b, c, and d |
b, c, d...all but WBC
|
|
|
1) A 40-year old female visits her physician and complains about fatigue. She has had strong menstrual blood flow during the last year.Her blood analysis reveals the following:
CBC Patient Normal MCH 8.0 g/dL (12-15.6g/dL) MCV 45.4 (fL) 82.0-100.0 (fL) Which of the following do these values suggest: (choose a -chromic, -cytic diagnosis of the anemia) |
hypochromic, microcytic
|
|
|
Identify the morphology that matches the syndrome
Iron deficiency anemia Anemia of chronic disease Thalassemia Sideroblastic anemia Pernicious anemia Folate deficiency Vitamin B12 deficiency |
Macro/micro -cytic / hypo/hypo -chromic
Iron def = (- / -) chronic disease = (N / N) Thalassemia = (- / -) Sideroblastic anemia (- / -) Pernicious anemia (+ / N) Folate deficiency (+ / N) Vitamin B12 deficiency (+ /N) |
|
|
What are the two most commonly encountered anemias.
|
Iron deficiency and anemia of chronic disease
|
|
|
Select true and false of the following statements about thalassemia
1. Increased Hgb A2 suggests alpha thalassemia. 2. Increased Hgb A2 suggests beta thalassemia 3. Genetic testing can be used to diagnose thalassemia |
1. False, Hb A2 is (a2 b2); alpha thalssemia has less alpha globin, no effect on this
2.True, since there is less beta globin around, more of the normally unsual Hb A2 (a2 d2) is made 3. True, since it is an inherited disease |
|
|
A patient is anemic with microcytic hypochromic indices. A source of blood loss has not been identified. Would it be safe to start iron therapy if the patient’s insurance would not cover any additional lab studies?
What test would you order if you could? |
No. 20% of patients with anemia of chronic disease have a microcytic anemia and their serum iron levels can be decreased. Therefore, iron therapy would not be indicated and if given over a prolonged period could contribute to iron overload. Additional iron studies, particularly serum ferritin levels should be ordered to confirm a need for iron therapy.
|
|
|
Why would people with kidney disease develop anemia
|
Because the kidney produces erythropoietin
|
|
|
Define megaloblastic anemia (cause).
|
Defect in DNA synthesis, Resulting in unbalanced cell growth, impaired cell division, Mature cytoplasm, immature nucleus, larger cell volume
|
|
|
What is the role of vitamin B12 and folic acid in megaloblastic anemia?
|
Both are important for DNA synthesis, Vitamin B12is required to convert methyltetrahydrofolate into tetrahydrofolate. Folate is required at several steps of DNA synthesis. Folate is a donor of single carbon units, also important for amino acid synthesis
|
|
|
Why would you give vitamin B12 as an injection and not orally?
|
If the problem is vitamin B12 absorption due to lack of intrinsic factor (pernicious anemia) then it would not be absorbed if given orally
|
|
|
Why would vegans be at risk for megaloblastic anemia?
|
Vitamin B12 is produced by bacteria, found in animals
|
|
|
Could thalassemia or sickle cell anemia lead to hemolytic anemia?
|
thalassemia: to some extend because red blood cells are small and have a short half-life, sickle cell anemia for sure, deformed red blood cells
|
|
|
What causes elliptocytosis and spherocytosis
|
inherited membrane defects. Elliptocytosis: defect usually in spectrin, destabilizes the cytoskeletal scaffold of cells, spherocytosis: Defects in cytoskeleton (ankyrin or spectrin)
|
|
|
What is the difference between intrinsic and extrinsic hemolytic anemia?
|
Intrinsic is caused by endogenous factors, e.g. elliptocytosis, spherocytosis, or metabolism defects; extrinsic is due to external factors: e.g. infections, drug-induced
|
|
|
A patient of Mediterranean descent shows symptoms of mild anemia. What type of disorder do you suspect?
|
Thalassemia – minor Beta
|
|
|
A patient complaining about feeling tired and pale has a blood sample taken. The red blood cells appear microcytic and hypochromic. What type of anemia could explain these values? Explain why. What further tests would you suggest?
|
Iron deficiency anemia (Fe deficiency)
Test for serum ferritin |
|
|
Which of the conditions discussed in class would lead to normocytic, normochromic red blood cells that are reduced in numbers? Explain why.
|
hemolytic anemias
|
|
|
A patient has an overall reduced blood cell count. You suspect aplastic anemia. Which tests would you like to perform to confirm your diagnosis?
|
RBC count, reticulocyte count
|