Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
22 Cards in this Set
- Front
- Back
|
The pterion lies just above what aretery? A fractuure here can cause what?
|
Middle meningeal a - epidural hemorrhage.
|
|
|
Review N6 for location of Bregma, Naseon, Asterion, and Lambda
|
Review N6 for location of Bregma, Naseon, Asterion, and Lambda
|
|
|
Re lecture page 5, See important structures on N99, N101, N102
|
1. Both layers of dura mater
2. Falx cerebri - where dura folds on itself |
|
|
Anteriorly, what does the Falx cerebri connect to? What does it attach to posteriorly and laterally? (lecture pg 8)
|
Anterior: Crista Gali - coming up from the ethmoid.
Posterior/lateral: to the occipital bone along a protuberance that |
|
|
What dura/meninges layer lies above the cerbellum? What does it attach to?
|
Tentorium cerebelli (think Tent). Attaches to Anterior and Posterior Clinoid processes.
|
|
|
Name dura mater layer on N103
|
Falx Cerebri, Tentorium cerebelli, Diaphragma Sellae
|
|
|
What sits in the Hypophyseal fossa?
|
Pituitary gland.
|
|
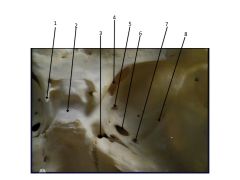
What is the groove all about?
|
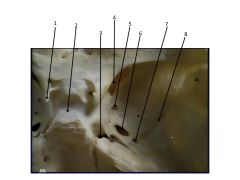
1. Anterior Clinoid
2. Sella Turcica 3. Foramen Lacerum 4. Superior orbital fissure 5. Foreman Rotundum 6. Foremen ovale 7. Foreman spinosum 8. Middle meningeal groove *The middle meningeal groove is where the artery lies - it originates from the Foreman spinosum |
|
|
See N102, NC1-74 for important structures. Also review, N103
|
See N102, NC1-74 for important structures. Also review N103
|
|
|
Review important structures on N101, lecture pg13
|
Review important structures on N101, lecture pg13
|
|
|
Describe an epidural hemorrhage. N101
|
Bleed bn endocranium (bone) and dura
|
|
|
Describe a Subdural hemorrhage N101
|
Bleed bn dura and arachnoid
|
|
|
Describe a Subarachnoid hemorrhage. What is a common symptom. N101
|
Bleed bn subarachnoid space. Sudden and severe headache.
|
|
|
Describe a Cerebral hemorrhage
|
Bleed within substance of the brain
|
|
|
What are the veins called that connect extracranial veins to intracranial veins?
|
Emissary veins.
|
|
|
Describe the four features of Emissary Veins
|
1. The connect extracranial & intracranial veins
2. Valveless 3. Blood flows in either directions 4. Facilitate spread of infection. |
|
|
Why are Emissary Veins prone to infection?
|
They're vavleless - so an infection on the scalp can enter the cranium and cause meningitis.
|
|
|
In addition to Emissary veins, what other two veins lead to the intracranial space? What are they thought to be useful for?
|
Superior and Inferior opthalamic viens. Thought to be a safety mechanism for an increase in pressure.
|
|
|
Describe the course of CSF. N108)
|
Chyloid plexus of 3rd ventricle makes CSf --> through cerebral aquiduct of Sylvius --> 4th ventricle (there's choroid here too) --> Exits via median aperature or foramen of Magendie --> circulate around spinal cord --> returns to venous system via arachnoid granulations.
|
|
|
What causes CSF volume increase (3)? What is this called? What are the types?
|
Causes:
1. Increased CSF production 2. Blockage of CSF circulation 3. Decreased CSF resorption Called Hydrocephalus Types: 1. Non-communicating 2. Communicating |
|
|
What does non-communicating type of hydrocephalus mean?
What about communicating hydrocephalus? |
Non-communicating: There's a blockage somewhere between the ventricular system and subarachnoid space. Perhaps due to a tumor near interventricular foremen of monroe.
Communicating: CSF can pass from ventricular system to subarachnoid space but it ain't leavin' or being resorbed. Perhaps caused by a tumor or infection |
|
|
What is the dialated space called where lumbar punctures are performed. At what location?
|
Lumbar cistern at L4/L5
|