Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
13 Cards in this Set
- Front
- Back
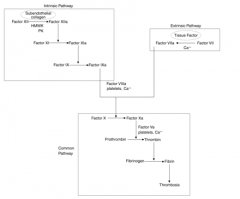
A 30-year-old male with Protein C deficiency sustains a large subarachnoid hemorrhage and bilateral calcaneus fractures after falling off of a roof. The patient has been in the intensive care unit for 5 days for monitoring of his head injury. All of the following factors are appropriate reasons to obtain a helical chest CT scan EXCEPT:
1. Elevated alveolar-arterial gradient (> 20 mm Hg) on arterial blood gas 2. Pulse oximetry reading of 99% with respiratory rate of 35 breaths/min 3. Pulse rate of 125 beats/min with new onset right bundle branch block 4. Paco2 > 35 mm Hg on arterial blood gas 5. Pao2 < 80 mm Hg on arterial blood gas |
All of the options listed except for Paco2 >35mmHg are indications of a pulmonary embolism. Most patients are hypoxic (Pao2 < 80 mm Hg), hypocapnic (Paco2 < 35 mm Hg), and have a high A-a gradient (> 20 mm Hg).
Pulse oximetry is not a reliable option to arterial blood gas measurements because patients can hyperventilate to maintain adequate oxygenation. Protein C deficiency is an inherited thrombophilia that increases the risk of venous thromboembolism(VTE). This patient is also at risk for VTE secondary to his sedentary status in the ICU and contraindication to administration of chemical VTE prophylaxis because of his subarachnoid hemorrhage.Ans4 |
|

A 35-year-old businessman complains of tingling and numbness in his fingers of both hands, mostly in the ring and small fingers, made worse with overhead activity. Neurologic exam and electromyography-nerve conduction study is normal. His cervical spine x-ray is shown in figure A. What is the most likely diagnosis?
1. C5-6 cervical disk herniation 2. C6-7 cervical disk herniation 3. bilateral cubital tunnel syndrome 4. bilateral radial tunnel syndrome 5. thoracic outlet syndrome |
The thoracic outlet space is created by the clavicle, first rib, subclavius muscle, costoclavicular ligament, and anterior scalene muscle. It most often affects subclavian artery, vein, and the lower trunk (C8 & T1) of the brachial plexus. The neurological exam may reveal sensory changes in the ring and little finger and intrinsic weakness. Radiographs here show cervical ribs, but could also show a Pancoast tumor or even be normal. Leffert reviewed thoracic outlet syndrome and cautioned that surgery be reserved for intolerable symptoms as surgical complications can be significant.Ans5
|
|

Which of the following templates, seen in Figures A-E, will increase the offset while keeping the leg lengths the same?
Answer 1: Figure A will decrease leg length and decrease offset. Answer 2: Figure B will maintain offset but decrease leg length. Answer 3: Figure C will decrease offset and maintain leg lengths. Answer 4: Figure D will increase leg length and increase offset. answer 5, Figure E the offset will be increased, while the leg lengths will remain unchanged |

Restoration of limb length is essential following total hip arthroplasty. The amount of limb-length change will be the vertical distance between the center of rotation of the femoral component and the center of rotation of the acetabular component. Thus, when the femoral center of rotation on templating is inferior to that of the acetabular component, the limb will be shortened. Restoring femoral offset is also important. If the center of rotation of the prosthetic head lies lateral to that of the cup on templating, the reconstruction will produce decreased offset.Ans5
|
|

Which of the following factors is most likely to increase the risk of hip dislocation after a total hip arthroplasty (THA)?
1. Large head-to-neck ratio 2. Use of a skirted femoral head 3. Femoral component in 15 degrees of anteversion 4. Acetabular cup in 15 degrees of anteversion 5. Acetabular cup in 50 degrees of abduction |
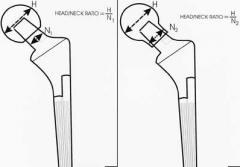
The use of a skirted femoral head actually decreases the head to neck ratio as seen in illustration A, and leads to increased risk of hip impingement and dislocation after THAs. Illustration B shows an example of a smaller head-to-neck ratio causing decreased hip arc of motion before impingement occurs.Ans2
|
|
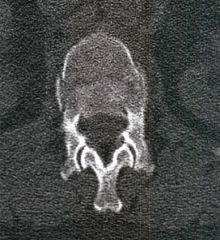
In a neurologically intact patient with the injury pattern shown in Figure A and B, what is the advantage of surgical treatment compared to early mobilization in a thoracolumbosacral orthosis?
1. Decreased kyphosis over time. 2. Decreased residual back pain. 3. Lower cost of hospitalization. 4. Earlier return to work. 5. No advantage - equivalent clinical outcomes |

The radiographs and CT scan show a burst fracture with minimal resultant kyphosis and minimal canal compromise. Because the patient is neurologically intact, and there is no evidence of injury to the posterior ligament complex (no increase in interspinous distance), the standard of care is to treat this injury nonoperatively with TLSO. If the patient had a neurologic deficit or clear injury to the PLC, as indicated by an increased interspinous distance or MRI showing ligament injury, then the treatment would be surgery with decompression and fusion.Ans5
|
|

A 29-year-old male presents with numbness and tingling in his lower extremities and gait instability for two weeks duration. Physical exam shows 3+ brisk patellar reflexes. Magnetic-resonance-imaging is shown in Figure A. What is the most appropriate first line of treatment?
1. Observation 2. Physical therapy 3. Epidural injection 4. Laminectomy 5. Anterior diskectomy |
The clinical presentation and imaging studies are consistent with a thoracic disk herniation with spinal cord compression causing symptoms of thoracic myelopathy. This is an indication for surgery. Thoracic level disk herniations are treated with anterior diskectomy with or without fusion. Ans5
|
|

A 47-year-old male presents with back pain of 2 weeks duration. He denies night sweats, fevers, or weight loss. He localizes his symptoms to a dermatomal distribution along the rib cage on the right. On physical exam he has mild paraspinal tenderness, normal patellar reflexes, normal muscle strength in his lower extremities, and a normal gait exam. An MRI is shown in Figure A and B. What is the most appropriate first step in management?
1. A repeat MRI with gadolinium 2. CT of chest, abdomen, and pelvis followed by a CT guided biopsy of the spinal lesion 3. Physical therapy and NSAIDs 4. Surgical decompression using a midline posterior approach 5. Surgical decompression using a transthoracic approach |
Because this patient has no neurologic deficits, surgery would not be indicated. Ans3
|
|

A 55-year-old woman undergoes endoscopic transthoracic anterior surgery for a herniated disk in the thorax. What is the most likely complication following surgery?
1. Increased kyphosis 2. Pseudarthrosis 3. Intercostal neuralgia 4. Pneumothorax 5. Cardiac tamponade |
In the cited study the authors address the surgical strategies required to resect residual herniated thoracic discs. Endoscopic surgery requires establishment of portals between the ribs and frequently causes compression of the intercostal nerves. Therefore, the most common complication is intercostal neuralgia. Pneumothorax and cardiac tamponade are extremely rare. Ans3
|
|

A 15-year-old female who is an avid runner has started developing increasing pain along her right leg. She indicates that the pain has developed in the past few months and has progressed in the past few weeks to where she can not tolerate weightbearing on the limb. She runs approximately 10 miles per day and is set on a collegiate running career. She notes that her menses began at age 11, but she has not had a menstrual cycle for 3 months presently. She denies sexual activity. On examination, she is exquisitely tender over the left tibia at the level of the distal third of the midshaft. Radiographs are seen below in Figure A and Figure B. What of the following should be included as part of this patient’s management?
1. Observation with continuation of physical activity 2. Discontinuation of running with WBAT in CAM walker 3. Intramedullary nailing of the tibia 4. Casting of the affected lower extremity 5. Discussion of eating habits and training regimens |
Based on the history, clinical presentation and the radiographs presented, the patient has developed a stress reaction of her anterior tibia. This is consistent with a diagnosis of female athletic triad. The next step needs to include a multifaceted treatment approach that includes psychological counseling, review of dietary intake and addressing her training habits that put her at risk for developing a stress fracture.Ans5
|
|
|
A 30-year-old male with Protein C deficiency sustains a large subarachnoid hemorrhage and bilateral calcaneus fractures after falling off of a roof. The patient has been in the intensive care unit for 5 days for monitoring of his head injury. All of the following factors are appropriate reasons to obtain a helical chest CT scan EXCEPT:
1. Elevated alveolar-arterial gradient (> 20 mm Hg) on arterial blood gas 2. Pulse oximetry reading of 99% with respiratory rate of 35 breaths/min 3. Pulse rate of 125 beats/min with new onset right bundle branch block 4. Paco2 > 35 mm Hg on arterial blood gas 5. Pao2 < 80 mm Hg on arterial blood gas |
All of the options listed except for Paco2 >35mmHg are indications of a pulmonary embolism. Most patients are hypoxic (Pao2 < 80 mm Hg), hypocapnic (Paco2 < 35 mm Hg), and have a high A-a gradient (> 20 mm Hg).
Pulse oximetry is not a reliable option to arterial blood gas measurements because patients can hyperventilate to maintain adequate oxygenation. Protein C deficiency is an inherited thrombophilia that increases the risk of venous thromboembolism(VTE). This patient is also at risk for VTE secondary to his sedentary status in the ICU and contraindication to administration of chemical VTE prophylaxis because of his subarachnoid hemorrhage.Ans4 |
|
|
A 30-year-old male with Protein C deficiency sustains a large subarachnoid hemorrhage and bilateral calcaneus fractures after falling off of a roof. The patient has been in the intensive care unit for 5 days for monitoring of his head injury. All of the following factors are appropriate reasons to obtain a helical chest CT scan EXCEPT:
1. Elevated alveolar-arterial gradient (> 20 mm Hg) on arterial blood gas 2. Pulse oximetry reading of 99% with respiratory rate of 35 breaths/min 3. Pulse rate of 125 beats/min with new onset right bundle branch block 4. Paco2 > 35 mm Hg on arterial blood gas 5. Pao2 < 80 mm Hg on arterial blood gas |
All of the options listed except for Paco2 >35mmHg are indications of a pulmonary embolism. Most patients are hypoxic (Pao2 < 80 mm Hg), hypocapnic (Paco2 < 35 mm Hg), and have a high A-a gradient (> 20 mm Hg).
Pulse oximetry is not a reliable option to arterial blood gas measurements because patients can hyperventilate to maintain adequate oxygenation. Protein C deficiency is an inherited thrombophilia that increases the risk of venous thromboembolism(VTE). This patient is also at risk for VTE secondary to his sedentary status in the ICU and contraindication to administration of chemical VTE prophylaxis because of his subarachnoid hemorrhage.Ans4 |
|
|
A 30-year-old male with Protein C deficiency sustains a large subarachnoid hemorrhage and bilateral calcaneus fractures after falling off of a roof. The patient has been in the intensive care unit for 5 days for monitoring of his head injury. All of the following factors are appropriate reasons to obtain a helical chest CT scan EXCEPT:
1. Elevated alveolar-arterial gradient (> 20 mm Hg) on arterial blood gas 2. Pulse oximetry reading of 99% with respiratory rate of 35 breaths/min 3. Pulse rate of 125 beats/min with new onset right bundle branch block 4. Paco2 > 35 mm Hg on arterial blood gas 5. Pao2 < 80 mm Hg on arterial blood gas |
All of the options listed except for Paco2 >35mmHg are indications of a pulmonary embolism. Most patients are hypoxic (Pao2 < 80 mm Hg), hypocapnic (Paco2 < 35 mm Hg), and have a high A-a gradient (> 20 mm Hg).
Pulse oximetry is not a reliable option to arterial blood gas measurements because patients can hyperventilate to maintain adequate oxygenation. Protein C deficiency is an inherited thrombophilia that increases the risk of venous thromboembolism(VTE). This patient is also at risk for VTE secondary to his sedentary status in the ICU and contraindication to administration of chemical VTE prophylaxis because of his subarachnoid hemorrhage.Ans4 |
|
|
A 30-year-old male with Protein C deficiency sustains a large subarachnoid hemorrhage and bilateral calcaneus fractures after falling off of a roof. The patient has been in the intensive care unit for 5 days for monitoring of his head injury. All of the following factors are appropriate reasons to obtain a helical chest CT scan EXCEPT:
1. Elevated alveolar-arterial gradient (> 20 mm Hg) on arterial blood gas 2. Pulse oximetry reading of 99% with respiratory rate of 35 breaths/min 3. Pulse rate of 125 beats/min with new onset right bundle branch block 4. Paco2 > 35 mm Hg on arterial blood gas 5. Pao2 < 80 mm Hg on arterial blood gas |
All of the options listed except for Paco2 >35mmHg are indications of a pulmonary embolism. Most patients are hypoxic (Pao2 < 80 mm Hg), hypocapnic (Paco2 < 35 mm Hg), and have a high A-a gradient (> 20 mm Hg).
Pulse oximetry is not a reliable option to arterial blood gas measurements because patients can hyperventilate to maintain adequate oxygenation. Protein C deficiency is an inherited thrombophilia that increases the risk of venous thromboembolism(VTE). This patient is also at risk for VTE secondary to his sedentary status in the ICU and contraindication to administration of chemical VTE prophylaxis because of his subarachnoid hemorrhage.Ans4 |