Reading...
![]()
Play button
![]()
Play button
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
5 Cards in this Set
- Front
- Back

Creation of a Stener lesion, as found in Gamekeeper's thumb, requires combined tears of the proper and accessory ulnar collateral lig in order for the ligament to be displaced by the adductor aponeurosis. Which describes the role these ulnar collateral ligaments (PCL/ACL) play in thumb MCP joint stability? 1-PCL is primary restraint to radial deviation with MCPJ in flexion, ACL provides restraint to radial deviation with MCPJ in exten 2-PCL is primary restraint to radial deviation with MCPJ in extension, ACL provides restraint to radial deviation with MCPJ in extension
3-ACL is primary restraint to ulnar deviation with MCPJ in flexion, PCL provides restraint to ulnar deviation with MCPJ in extension; 4-ACL is primary restraint to radial deviation with MCPJ in flexion, PCL provides restraint to radial deviation with MCPJ in extension; 5-PCL is primary restraint to ulnar deviation with MCPJ in flexion, ACL provides restraint to radial deviation with MCPJ in extension |

The proper ulnar collateral ligament(PCL) runs from the metacarpal head to the volar aspect of proximal phalanx and resists ulnar stress with the thumb MCPJ in flexion. The accessory ulnar collateral ligament(ACL) lies palmar to the proper ligament, and insets inserts onto the volar plate. The volar plate and ACL function as the principle restraints to ulnar stress with the thumb MCPJ in extension, Newland, in his review article on Gamekeeper's Thumb, states that criteria for judging what constitutes a complete tear vary from 15 deg to 45 deg difference with respect to the opposite side. He goes on to state, however, that many authors choose an absolute value of >35 degrees of joint laxity compared to the contralateral side when judging a tear to be complete or incomplete. When an acute tear is identified, surgical repair is recommended.Ans1
|
|

Hx:30yo F undergoes arthroscopy for a chronically painful R wrist that failed to improve w/4 mths of immobilization & NSAIDS, PE= revealed point tenderness dorsally over the lunate but no tenderness elsewhere in the wrist. on scope see a chondral flap. The articular surface of the lunate is stable to probing. xray & MRI image of the pts wrist Fig B & C. What is the next step in tx? 1-Continue Immobilization and NSAIDS; 2-Radial shortening osteotomy; 3-Proximal row carpectomy; 4-STT fusion; 5-Wrist fusion
|

consistent with Stage 2 Kienbock's dz in the setting of (-)ulnar variance. Radial shortening osteotomy is the most appropriate treatment option listed for Stage 2 dz= lunate sclerosis w/out significant collapse. Shortening osteotomy can alter DRUJ contact pressures leading to remodeling, especially in the presence of a Tolat Type II DRUJ, such as that shown in the radiographs. However, this remodeling has been shown to occur without the development of arthritis, and therefore is not a contraindication to this procedure, This patients xrays shows some slight sclerosis of the lunate and negative ulnar variance, and the MRI shows diffuse edema and early osteonecrosis of the lunate. The arthroscopic image shows a cartilage flap with a stable base left on the lunate. Based on these images, the patient has Stage 2 dz and should be treated with a joint leveling procedure; or radial shortening osteotomy in this case. Incorrect Answers:
Answer 1: Immobilization and NSAIDS is indicated in Stage I disease or as a first line of treatment for Stage 2, which this patient has failed. Answer 3: Proximal row carpectomy is indicated in Stage 3B. Answer 4: STT Fusion is indicated in Stage 3B. Answer 5: Wrist fusion is indicated in Stage 4.Ans2 |
|
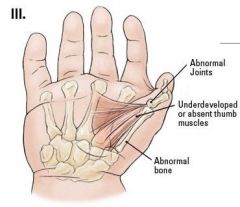
Using the Blauth classification of thumb hypoplasia, grade IIIA can be txd w/ thumb reconstruction whereas grade IIIB is treated with thumb amputation & pollicization. What is the key difference between these two grades? 1-presence of complete osseous structures; 2-presence of intact musculotendinous structures, 3-CMC jt stability;4-MCP jt stability
5. presence of an EPL tendon |
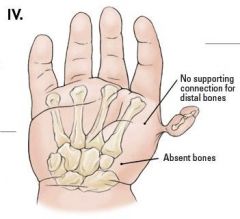
To function correctly, the thumb must be positioned so that it can oppose the adjacent medial fingers and grasp objects securely from an antiposed (abducted, slightly extended, and pronated) position. Although normal motion is usually not required at the MP or interphalangeal joints, thumb function is greatly dependent on preserving a full arc of circumduction at the carpometacarpal (CMC) joint. The CMC joint must be sufficiently stable to provide resistance during grasp and pinch. The Blauth's classification ranges from type I to V and Types IIIB to V are treated with pollicization. The key difference between a Blauth IIIA and IIIB is the presence of carpometacarpal joint stability in Blauth IIIA.Ans3
|
|

Hx:68yo F office assistant reports L thumb pain that has progressively worsened x 2 yrs, L hand dominant and reports difficulty with opening jars and holding a coffee cup. PE=L hand she has a (+) thumb CMC grind test and has a fixed deformity at the thumb MCP jnt. Fig A demonstrates the left hand grasping an object and Fig B xray, What is the next step in tx? 1-Carpometacarpal joint fusion and MCP jnt volar capsulodesis; 2-CMC jnt resection arthroplasty and MCP joint volar capsulodesis
3-CMC jnt resection arthroplasty and MCP jnt fusion 4-CMC jnt resection arthroplasty and temporary MCP joint perc pin fix; 5-CMC jnt fusion and MCP joint fusion |

hx, PE, and images are consistent with thumb CMC (basilar) joint arthritis with associated MCP joint arthritis. At the MCP joint there is hyperextension of the thumb metacarpophalangeal (MCP) joint and adduction involving the first web space of the hand (Z deformity). Arthrodesis of the MCP joint is the treatment of choice when thumb MCP hyperextension exceeds 40°, the deformity is not passively correctable, or advanced degenerative changes are noted to affect the articulation.
when MCP joint hyperextension is: 0° to 10°= Surgical intervention is not necessary when MCP hyperextension is less than 10°. 10° to 20°= Percutaneous pinning of the MCP joint in 25° to 35° of flexion for 3-4 weeks may be performed independently or as an adjunct to EPB transfer. 20° to 40°= Capsulodesis of the volar aspect of the MCP joint is recommened to provide a check rein for hyperextension and Sesamoidesis has also been investigated as an adjunctive procedure.Ans3 |
|

A 60-year-old man has chronic pain at the base of this thumb and weakness on attempted thumb pinch. A radiograph is shown in Figure A. Which injection would likely reduce his pain and increase his function? Topic Review Topic
FIGURES: A QID: 2935 1. Saline 2. Steroid 3. Hylan 4. All of the above are equally effective 5. All of the above are detrimental |
The patient has basal joint arthritis of the thumb and randomized controlled trials have failed to demonstrate an advantage of steroid or hylan over saline.Ans 4
|