![]()
![]()
![]()
Use LEFT and RIGHT arrow keys to navigate between flashcards;
Use UP and DOWN arrow keys to flip the card;
H to show hint;
A reads text to speech;
12 Cards in this Set
- Front
- Back
Integrated endocrine physiology - Growth & development system - Reproductive system - Maintenance of internal environment |
A hormone may exert more than one action E.g. Insulin actions on metabolism. Acts on many different tissues, with many different actions- can promote growth etc. A single function may be regulated by several hormones E.g. lipolysis. Inhibited by insulin, stimulated by glucagon, cortisol, GH's, catecholamines etc. Hormones act with other hormone |
|
|
Synergistic hormones |
Produce a much greater enhanced response than the sum of either of the hormones alone - Thyroid hormones on the activity of catecholamines/sympathetic NS. Upregulate expression of β-adrenoceptors - CRH & AVP on ACTH release- both act on ant pituitary in fluid deprivation - Cortisol & growth hormone on metabolism |
|
|
Permissive hormones |
Presence of one hormone allows a second hormone to act E.g. cortisol on catecholamine activity E.g. thyroid hormones on growth hormone activity in growth promotion |
|
Growth & development |
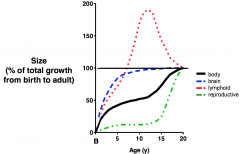
Structural growth is net protein synthesis, lengthening of bones, ↑ no & size of cells NOT weight gain, which is due to fat & water accumulation - Highest growth rate = foetal development & just after birth (first 2 yrs) - Further growth spurt occurs at puberty Major brain development in early adulthood Lymphoid system development peaks in adolescence due to exposure of antigens Reproductive system majorly develops in puberty |
|
|
Factors that contribute to growth |
1. GENETIC- correlation btw parental & offspring height 2. SOCIOECONOMIC & NUTRITION- poverty, hygiene, malnutrition 3. CHRONIC DISEASE & STRESS- malabsorption, cortisol = anti-growth 4. ENDOCRINE HORMONES- mainly GH, also insulin, thyroid hormones, glucocorticoids, sex hormones |
|
|
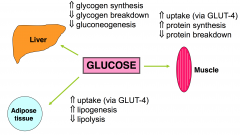
Actions of growth hormone - Major role in growth & metabolism |
Direct on METABOLISM. Increases lipolysis, increases aa uptake & protein synthesis, increases hepatic glucose output (gluconeogenesis) & decreases glucose uptake ANTI-INSULIN- shift of source of fuel from CHO's to fats. Synergism between cortisol & growth hormone Indirect, promotes GROWTH. Stimulates release of other growth factors e.g. IGF-I & IGF-II (somatomedins) from liver & other cells. Growth via IGF-I = protein synthesis & hypertrophy, cell division & hyperplasia, skeletal growth (height increase). Requires thyroid hormone presence |
|
|
Other key hormones for growth |
- THYROID HORMONES- permissive role on growth hormone activity. Key role in CNS development - INSULIN- anabolic growth promoter - SEX HORMONES- ↑ [conc] during puberty, causing linear growth, muscle building, & stops bone elongation by promoting epiphyseal plate closure |
|
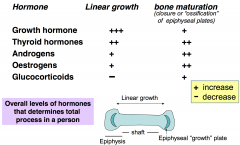
Long bone growth |
At the end of adolescence due to sex hormones, ossification of epiphyseal growth plates occur. Bones then cannot lengthen further, despite presence of growth hormones - Glucocorticoids promote bone maturation ∴ chronic stress causes inhibition of linear growth & bone maturation |
|
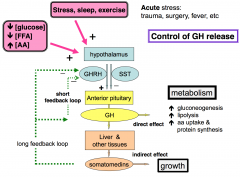
Control of growth hormone release |
Ant pituitary hormones exert trophic effects on specific tissues e.g. prolactin-breast, LH/FSH-gonads, TSH-thyroid, ACTH-adrenal cortex - Growth hormone releasing hormone (GHRH) increases release - Somatostatin (SST) inhibits release ∼70% of total daily GH is released during sleep Secretions high during childhood, peak at puberty, & fall during adulthood |
|
|
Glucocorticoids & growth hormone |
Dual effect - Initial synergism on metabolism- both ↑ gluconeogenesis & lipolysis - Chronic high [glucocorticoids] inhibits GH release e.g. Cushing's syndrome, long-term use of steroids |
|
|
Disturbances in the endocrine system Stunted growth - Pituitary dwarfism- GH deficiency, reduces long bone growth - Hypothyroidism- reduces thyroid hormones for GH activity - Cushing's syndrome - Congenital adrenal hyperplasia & sexual precocity- ↑ androgens cause early ossification of epiphyseal plates |
Growth hormone deficiency in adulthood - Variety of non-specific symptoms e.g. physiological changes, malaise, tiredness, depression, osteoporosis, poor muscular tone, impaired hair growth, increase in adipose tissue Treat with recombinant human growth hormone (HGH) |
|
|
Disturbances in the endocrine system Accelerated growth - Gigantism- tumour with GH secretion - Hyperthyroidism- excess thyroid hormones - Sexual precocity- initially accelerated linear bone growth, final adult heigh is short due to early bone growth maturation - Eunuchoidism- hypogonadism, reduced sex hormones delays bone maturation |
Acromegaly = excess GH in adulthood due to GH-secreting tumour - Coarsening of facial features, enlarged hands & feet, headaches & vision disturbances, tiredness, hypertension, cardiomegaly, diabetes, loss of periods Treat with surgery/radiotherapy, or inhibit GH release with SST analogues |